With covidminute.com, live from Shanghai
The news catches up with us, and I was asked, by readers in France and China, to try to “give meaning” to the “Covid” information.
🇫🇷 France : dashboard
Equation to dimensions: have in mind the “maximum figures” observed during the April peak:
- Hospitalizations (+4281) / Versus +54 today (but reporting WE)
- Intensive care (+771) / Versus +36 today (but reporting WE)
- Death (+ 605 at the Hospital) / Versus +81 today (but reporting WE)
🇫🇷 France : local gestion
The virus circulates in France and in the DOM, and an epidemic phase is observed according to the regions (IDF, North, …)
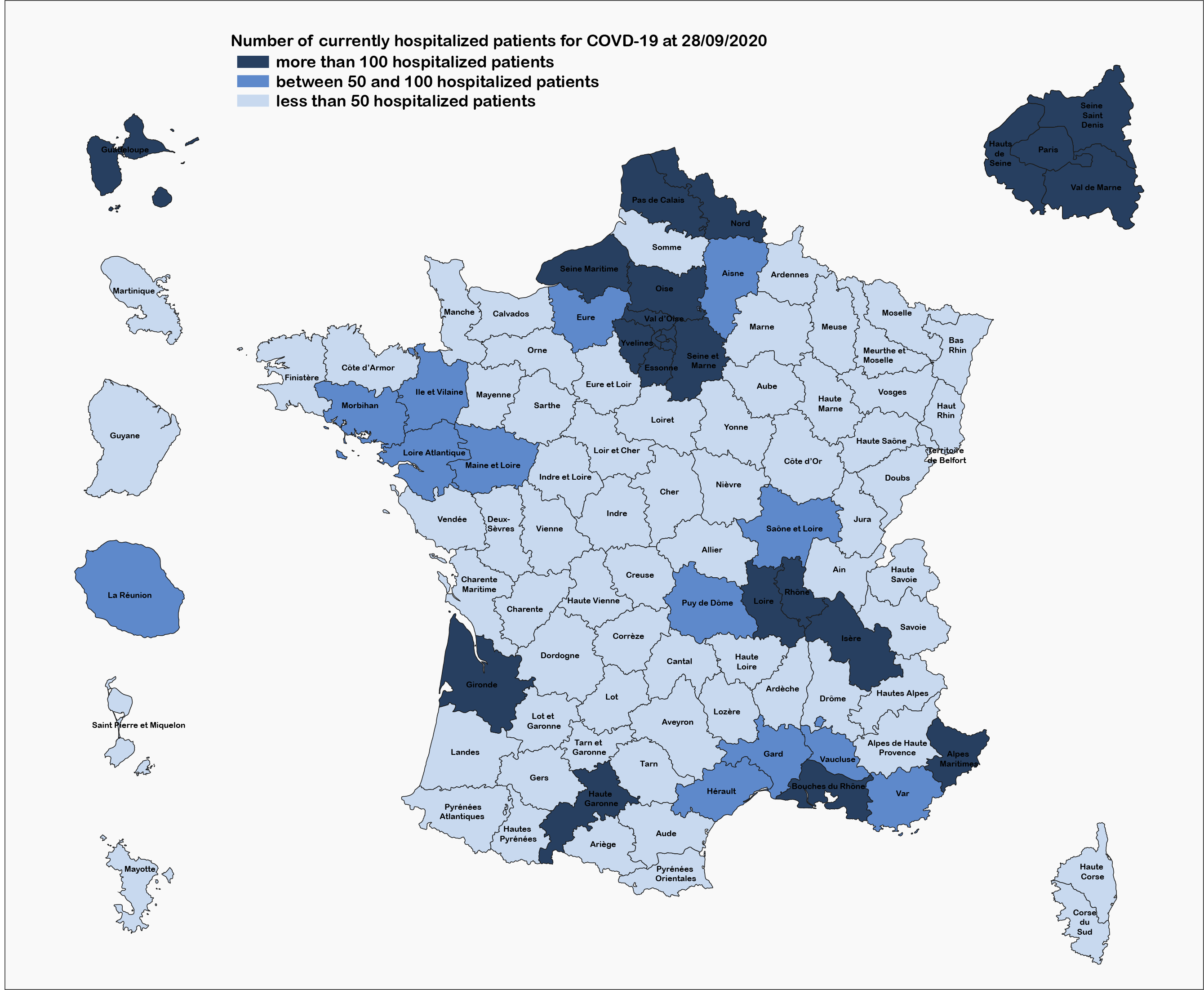
Source : Santé Publique France
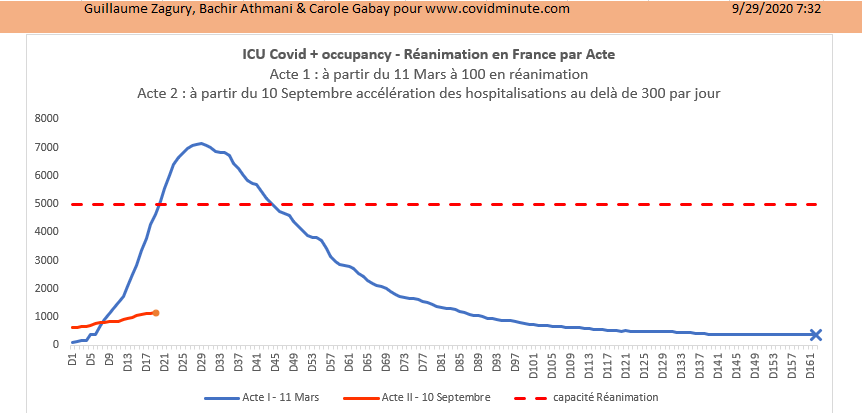
To understand the situation in France it is necessary to know how to reason on the issue – the reaniation beds, in terms of load/capacity (while knowing the cinetic decalee of 5 days, compared to symptomatic Cs):
“To govern is to predict”, and we understand better why the government is worried about our health system, which saved the day, last April: 5 main questions.
Increase in C (+) in progress (see rate of positivity, etc.), with its corollary on the probable hospital pressure, in the days to come.
Probable increase in C (-) to come in intensive care, following organic decompensations of autumn-winter virus diseases (influenza, gastroenteritis, etc.)
Unlike Germany (20,000 resuscitation beds), the French Health System (formerly considered one of the best in the world …), does not have the capacity to absorb a new massive flow (5,000 basic beds + / – possibility of increasing to 12,000 beds, “by pushing the walls”). This observation was already prior in pre-Covid, and it must be recognized that the dynamic of the current government is to change this state of affairs.
Regional allocation with variable geometry (load / capacity): thus some intensive care patients in the South of France, would already be transferred to IDF (a confirmer)
At European level: France is one of the countries whose indicators ask our colleagues (see appendix 5)
Consequently, everything depends on the evolution, and the effectiveness of the preventive measures to “flatten as much as possible” the curve (act 2 – red), and thus to be able to “live with” (while waiting for a vaccine?).
Hence the interest of educating the population with citizen and simple educational tools, like the one we present with my colleague Dr Athmani (see below), and thus to do everything to avoid a re-containment (see: 116% of public debt expected at the end of the year).
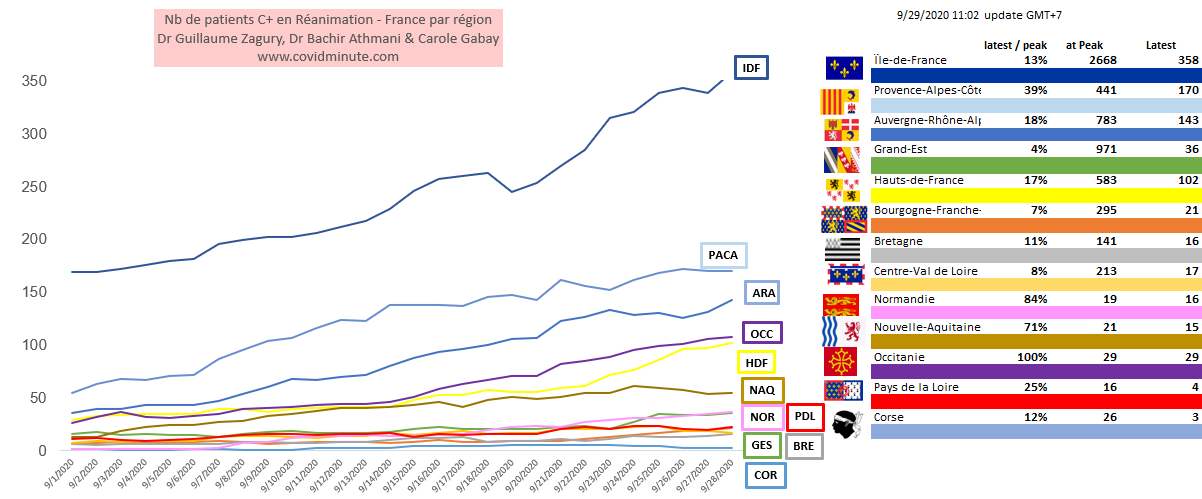
At regional level: it is necessary to think about C (+) patients AND C (-) patients in intensive care, to understand the stake (saturation of services). Note that some figures are difficult to obtain in real time.
note that resuscitations in Guadeloupe and Occitania are 100% full (see appendix)
Between the health risk (and its freedom-killing measures) and the economic risk (certain measures must be socially supported if they are to be taken as a last resort, following epidemiological figures….), The choice is extremely complex (still too early, to have all the “valid” figures on the impact of certain measures!), and is not new, neither in time nor in space. As the Governor of Hong Kong said in 2003 during the crisis du Sars: “We will die of economic death, before dying of biological death …”. The ideal is to respect preventive measures, both for vulnerable populations (+/- 20M in France), and for the general population.
⚠️ To go further
1/ Chronological Vision (Time)
2 & 3/ Regional Barometer & DOM TOM
🇪🇺 Europe : “Barometer per country”
A North South gradient observed
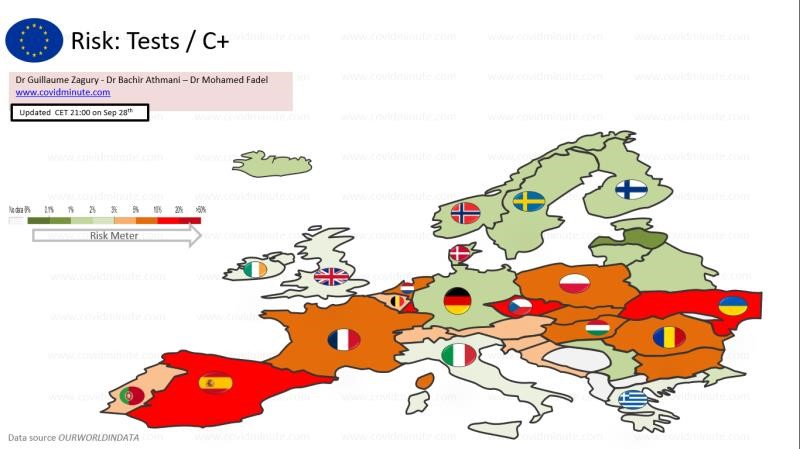
7 countries are currently “sensitive” in Europe: Spain and France in the south and some countries in the East (Romania, Czech Republic, Ukraine, etc.)
In terms of “homogeneous” comparisons, let us not forget that we must reason at 4 levels: local (department) – regional – national – European (note in table 5: we have shown the European average horizontally).
⚠️ To go further
World : “World pandemy”
Time : A 5 kinetic viral phase
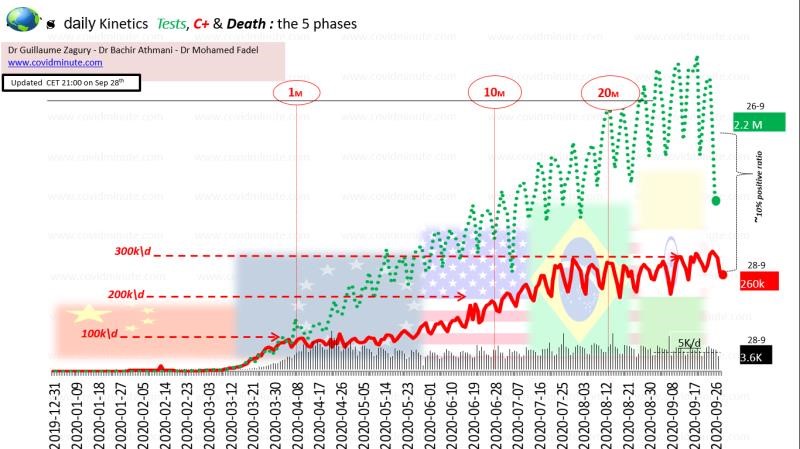
Have the few key figures in mind: 5k deaths / day and +/- 300k new officially declared C + / day (beware of everything that is “test dependent” in terms of measurement and interpretation).
Note the volatility of the figures during the WE, and we will see tomorrow, if the exact figures for the 3 main countries (see 4.2) are confirmed (also annex 7).
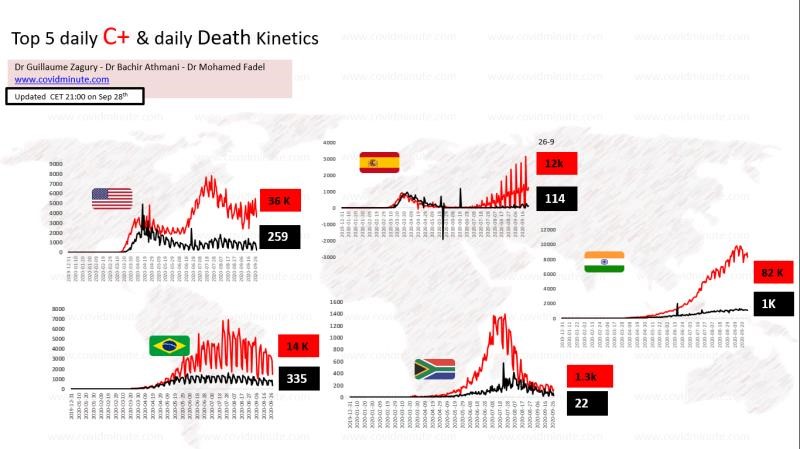
Space: India takes over from the Americas …
⚠️To go further:
6/ Kinetic deaths for major epidemic countries
« Out of the box » (weekly zoom)
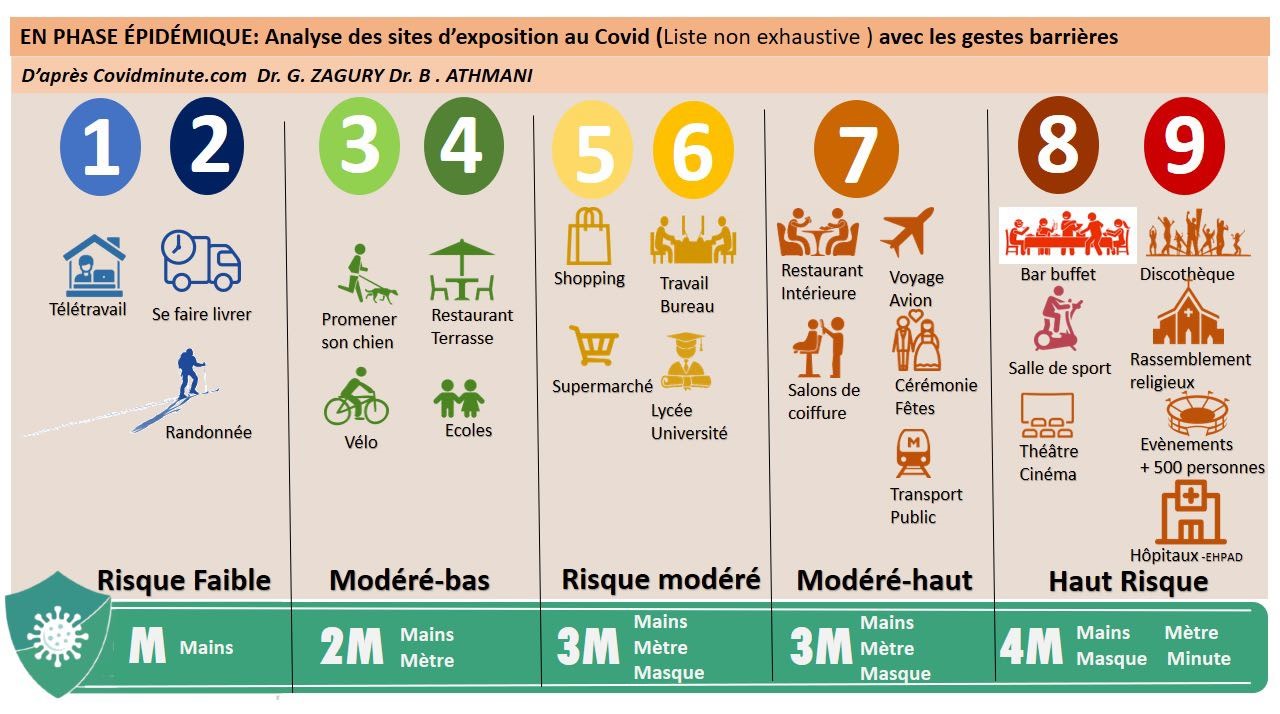
We offer a pedagogical tool for individual citizen prevention: possibility of evolving in places at risk, … on condition of an adapted and responsible individual behavior. We must also take into account current or future epidemiological data (cf. re-defining before the start of 3 major religious festivals).
Note that the “scientific” aspect can still be questionable (as for the masks in France initially!), And we base ourselves on our experience (proof of level 1 :-)) … Indeed, the time to put in The place of impact measurement tools is long (still few scientific articles measuring the risks accurately and quantified), but this will be done in the coming months …
💢
Géopathologie : « viral RNA expresses The Cultural DNA of Societies »
Global Technology Leadership: The little red book has turned pink?
I give you an appointment tomorrow, to finalize this chapter.
In the age of the “information highways”, relayed by social networks, our goal is thus to “return to the fundamentals”: to bring out daily 5-6 “strong signals”, factual rather than emotional, in the “noise” surrounding, and thus reassure the greatest number, in the face of a pandemic always evolutionary.
« All success is collective and so thank you to our teams (Dr. Bachir Athmani, Carole Gabay, Richard Coffre,…), as well as to our patrons, and of course to the Paul Benetot Foundation/Matmut Group.
– To follow…
Protect the most vulnerable with a “citizen” attitude
- 3M for the general population (70%)

- 4M for at-risk and most at-risk populations (30%)
See you tomorrow
Dr Guillaume Zagury
International Public Health Specialist
HEC
In China for 20 years
