Doctor Guillaume Zagury, based in Shanghai and specialist in international public health and “health innovations”, comments on a daily basis the evolution of the epidemic for more than 2 months, and gives us a preview of the elements of understanding on its “country analysis” and the foreseeable consequences (experiences of SARS in 2003 and Covid in China for 3 months).
A whole remarkable multidisciplinary volunteer team allows this factual and objective analysis to be carried out (by the way don’t hesitate to join us): “each success is collective”. Our new site will be launched at the beginning of the week and you will be able to put faces on the names.
A. France is moving towards collective immunity “suffered” and not “chosen”
1. The facts: not a peak, but a (long) plateau!
France follows a path similar to Italy. The number of intensive care patients in Italy has tended to decrease for a few days (similarly in France for 2 days, a trend which remains to be confirmed), but this decrease is taking place slowly, and for the time being Italy is not planning any end of lockdown in the next 3 weeks.
Chart: France-Italy comparison of deaths and intensive care patients

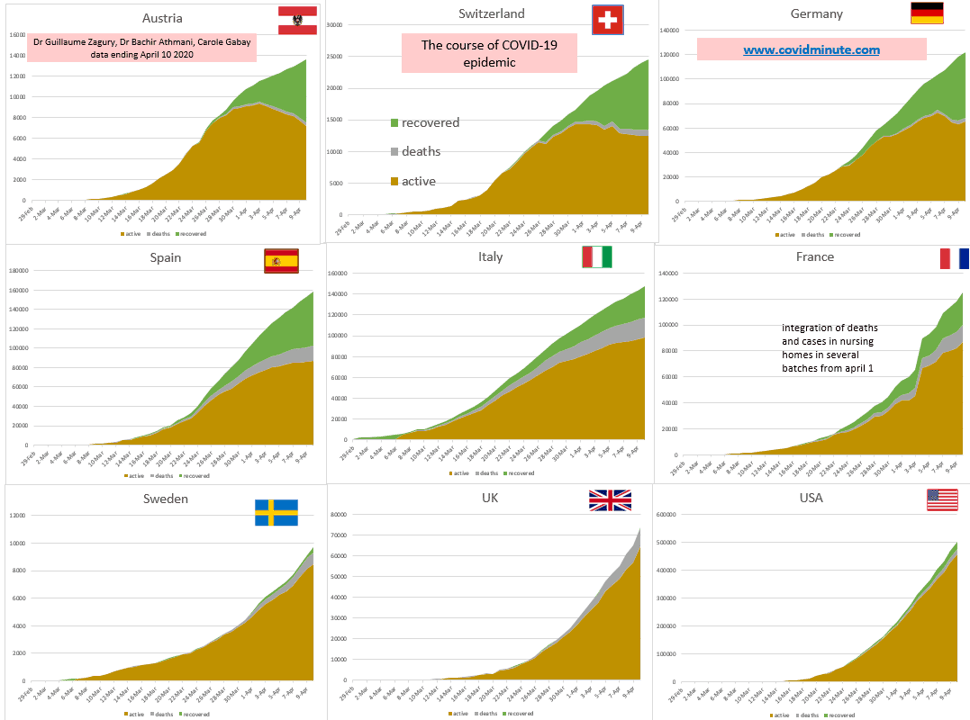
Chart: comparison with the main western countries

2. Generalized “flexible” lockdown: only one part of the arsenal!
Everything is said in our table CovidScore (tool that we created 3 weeks ago), which you will find in part B.
Our scoring is updated according to the measures implemented or planned by the authorities, evolving daily. For each country, we remind in the first column the measures at the time of the appearance of the first 100 cases, to see how the measures taken (“4M”, “3T”, intensive care beds available,…) impacted in time and space (comparison with Asian countries, themselves very preventive).
3. Interest of current lockdown only: limiting saturation of the health system
The current lockdown has been a very good measure for our health system to avoid rupture, as shown in the following diagram (for 2-3 days the balance between entries and exits in intensive care is slightly negative: -34 nationwide yesterday , but with saturation zones such as Paris region…).
Graph: evolution of I / O in intensive care

Without lockdown (which begins to have its effect after around 15-20 days), our healthcare system would have “exploded” because of the flow of patients in intensive care, despite the passage from 5 000 beds initially to 9 000 beds (for a current use of approximately 7 000 units).

4. Be realistic: status quo is not a long-term solution
Even if the lockdown currently in force in France is much more flexible than in Wuhan (where strict lockdown was maintained for 76 days), it cannot be kept in the long term:
– economic and social risk: as the Prime Minister of Singapore said in 2003 at the time of SARS, “we will die first of economic death, before dying of SARS!
– mental risk: 30% increase in domestic violence, psychological consequences of prolonged lockdown (studies in progress in China)
– health risk (“loss of opportunity”): chronic patients are very little followed up (unless they are affected by Covid-19, and same is true of screening of other conditions (“loss of opportunity” in oncology, …).
5. A solution must be found and prepared now with our current means
5.1. We know the disease: it is neither Ebola, nor AIDS, but a respiratory virus which can make certain fragile patients (which we must protect) decompensate.
Remember that Ebola mortality is over 50% (all ages), and that AIDS causes around 1 million deaths per year (2019 figures) worldwide.
The Covid risk factors are now well identified (distribution of mortality by age and comorbidities). The populations at risk must be constantly in our thoughts.

Research teams are working to elucidate a few unknowns. These include: the host animal, the immune status (current experience in Germany on 100 000 individuals, in order to have a map of their antibodies in time and space to discuss with quantitative data of natural immunity), endemic or cyclic (seasonal?) virus, new therapeutic progress (interleukins, …), possibility of an effective vaccine (a priori feasible, but not yet certain: let’s not forget that there is still no HIV vaccine).
5.2. Our current means: we are not Germany, which can deploy a much better preventive and curative arsenal (see table CovidScore in B).
Germany (5 times less deaths than France to date, while the epidemic seems to be decelerating) is one step ahead of us:
– it has certain key tools for obtaining a high “CovidScore” classification: masks, tests (the country has all the reagents, both PCR and serological), intensive care beds (more than 20k before the start of the epidemic, against 9k in France at present), ventilators (Germany exports…).
– it is independent on a large part of the necessary tools: it can rely on a “mid-range” industry which it has managed to preserve, while France is rather positioned in high tech industries, such as space.
– it was very reactive: in the CovidScore table, it went very quickly from group C to group A.
France has certainly placed orders (masks, tests, …) with many announcements, but the reality is there: we depend too much on Asia and the 2 billion masks have certainly been ordered, but their delivery will be random (date / health diplomacy, …).
Our industry (masks, biology, applications, ventilators, …) is evolving but would benefit from being more reactive (delays in the validation and regulatory processes).
We are not there to look back and redo the match, but to seek solutions that are within our means.
6. Controlled end of lockdown (progressive, regional, etc.) along 3 axes, with permanent monitoring: collective immunity “chosen” (living with) rather than suffered

B. CovidScore and CovExit: daily update
CovidScore: assessment of measures taken to stem the epidemic

CovExit: degree of preparation for end of lockdown

C. France and the world: more than 100 000 deaths in 3 months and more than 1.2 million active cases
With the contribution of Mathieu Bouquet and Stéphane, companions from the beginning, whom I thank again for their unfailing support.
1. Be cautious with the figures: extremely questionable!
The definition of the cases is too variable from one country to another, with measurement biases and therefore major under-declarations:
– many forms that are light or not symptomatic: in some countries, especially in the West and in France, these cases will not be counted, whereas they are in other countries, notably Asian.
– under test equipment: Africa, among others, has only a few positive cases, but probably mainly due to lack of tests
Predictive models are therefore to be taken with caution, as they are based on estimates that only very partially reflect reality.
Similarly, there are many biases in counting deaths: declaration (hospital and extra-hospital mortality in France, versus hospital mortality in Italy), or measurement (after death biological tests carried out or not, filling in certificates with the initial or secondary cause, etc.).
In our view, only certain relatively objective data such as the number of Covid patients in intensive care are relevant parameters to follow.
2. Prevalence: 1.22 million active cases confirmed under observation

Geographical distribution

Source : John Hopkins University
Top 10 countries
USA 457k
Italy 98k
France and Spain 87k
UK and Germany 65k
Turkey 44k
Iran 28k
Russia, Brazil, Canada, Portugal, Netherlands, Belgium, Switzerland : 10 à 20k
By continent: 82% of cases diagnosed in Western countries

3. Incidence: 96k new cases diagnosed (85k yesterday) and an epidemic wave still going west
Chart: evolution of the number of new daily cases

By country: note that the number of cases diagnosed is an indicator to be taken with caution (thus the USA launch massive campaigns of screening tests and therefore display figures in much higher proportion than many European countries which have very few tests).
USA 34k (+5k)
Spain 5k (+0k)
UK 9k (+5k)
Germany 4k (-0k)
France 7k (+2k)
Italy 4k (+0k)
Turkey 5k (+1k)
Iran 2k (-0k)
Ecuador, Chile, Peru, Brazil, Canada, India, Russia, Ireland, Netherlands, Belgium, Switzerland; Sweden : 1 to 2k

By continent: 3 outbreaks – USA, Europe and Middle East

Chart: evolution of the number of new cases by country (beware of measurement bias: see USA massive tests)
4. Intensive care and mortality compared according to time and space (for information)
4.1. Intensive care cases

4.2. Daily mortality
Like other figures, this indicator is questionable: in some countries, the mortality is only recorded in hospitals (as in Italy initially) due to the lack of tests or initial disorganization, while in others it is both hospital and extra-hospital as in France.

5. Full evolutive tables for figures lovers
Incidence evolution in the 11 most affected areas

French regions: slight overall improvement, but Ile de France is still under tension

Virus Preventions 4 W’s:
Wear a mask, Wash your hands, Watch out for sick people, Wait for new updates from covidminute.com !
Protect yourselves, and above all protect the most vulnerable!
Dr. Guillaume ZAGURY,
Specialist in Public Health and Health Innovations
Consultant at “Health Innovations”
HEC
In China for 20 years“All success is collective”, thanks to:
– the whole “Back Up” team (Mathieu Bousquet, Carole Gabay, Flavien, Marie, Laetitia, Anne-Sophie, …), without whom this project would not have been possible.
– all the “Medical” team (Dr Bachir Athmani, Dr Ibrahim Souare, Dr Taieb, Dr Viateur …) who allow this project to exist,
– all historical financial sponsors (Jerome, Benjamin Denis & B Square, Benoit Rossignol, Arnault Bricout) who work for “Citizen Actions”
If you feel like a patron or of partners to finance IT development, don’t hesitate to contact me (guillaume@covidminute.com).
Also, even if part of the team is based in Shanghai, do not hesitate to come and join us, because there is no shortage of work :-)If you want to find more analyses and infographics, follow our account at:Know the latest updates
Powered byMedicilline