With covidminute.com, live from Shanghai
The news catches up with us, and I was asked, by readers in France and China, to try to “give meaning” to the “Covid” information.
🇫🇷 France : dashboard
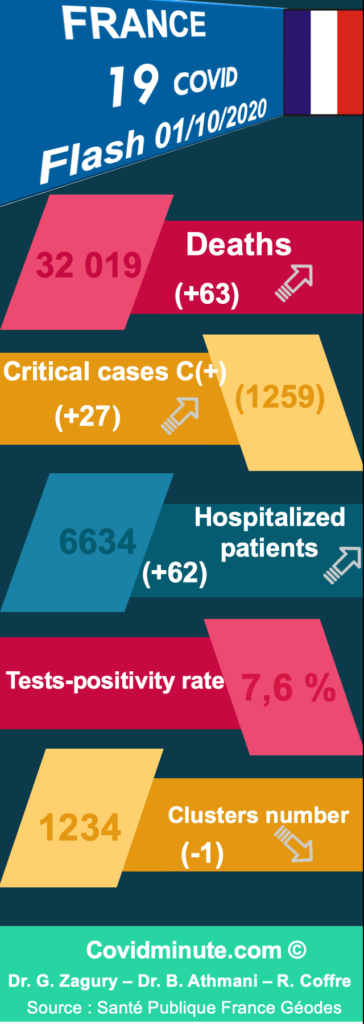
Equation to dimensions: have in mind the “maximum figures” observed during the April peak:
- Hospitalizations C+ no ICU (32.131) / Versus 5352 today
- Intensive care (7632) / Versus 1265 today
- Death (+ 605 at the Hospital) / Versus +63 today
🇫🇷 France : local gestion
Unlike phase 1 where an east-west gradient was observed, the virus circulates in more than 70% of the territory and in the overseas departments, and an epidemic phase is observed depending on the region (IDF, North, etc.)
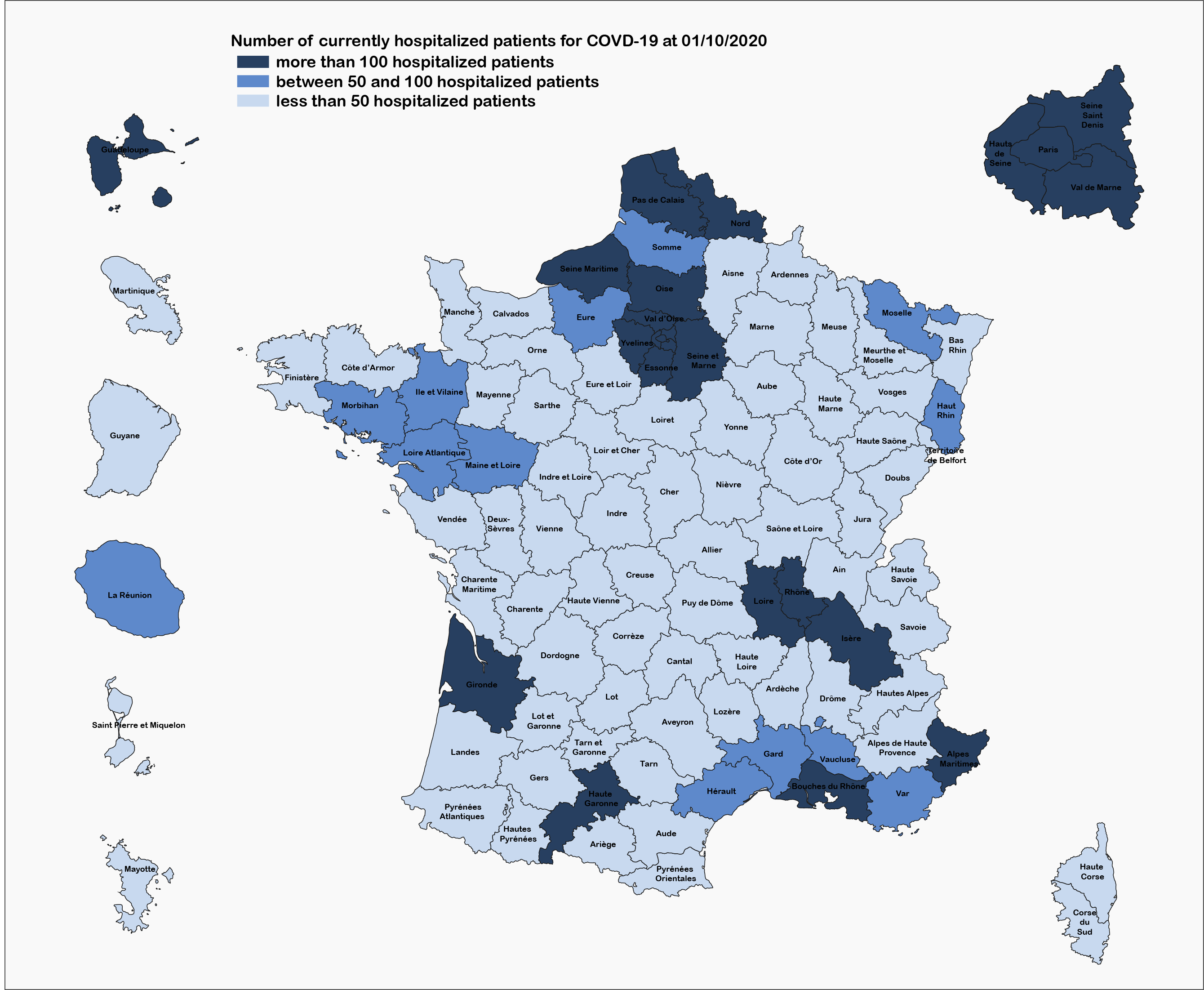
Source : Santé Publique France
To understand the situation in France, you have to know how to reason about the issue = intensive care beds, in terms of load / capacity.
On a national level:
In terms of load capacity, we know that the situation was already very tense in autumn-winter in pre-Covid
Unlike phase 1:
Resuscitations fill up very gradually
We are in the emergence phase of autumnal viruses and their organic decompensations are and will also be taken care of, in addition to “classic” C (-) patients (heart attack, attempted suicide, etc.)
To create beds, equipment is certainly needed, but above all human resources (doctors, nurses, nursing assistants, etc.)
In terms of human resources (one of the keys):
The transfer of caregivers is more delicate because the West and the South are also affected, which was not the case in phase 1.
A physical and moral weariness to “put it back” can be observed among caregivers.
Consequently, we understand better, why the government is doing everything to “flatten the curve”, and thus avoid at all costs a situation of reconfinement (cf Israel, +/- Madrid)

Note that the 30% threshold (“alert”) applies in addition to the 2 test positivity indicators (quantitative and qualitative C + & C + 70+), at the regional level above all. We are also using it at the national level, so as to “fix ideas” on key ratios.
Some regions (in particular IDF) are already under tension and note that in Paris some resuscitations are 40% of C + patients.
We are preparing a more meaningful iconography than this one, which already has the merit of existing and of giving a regional trend.
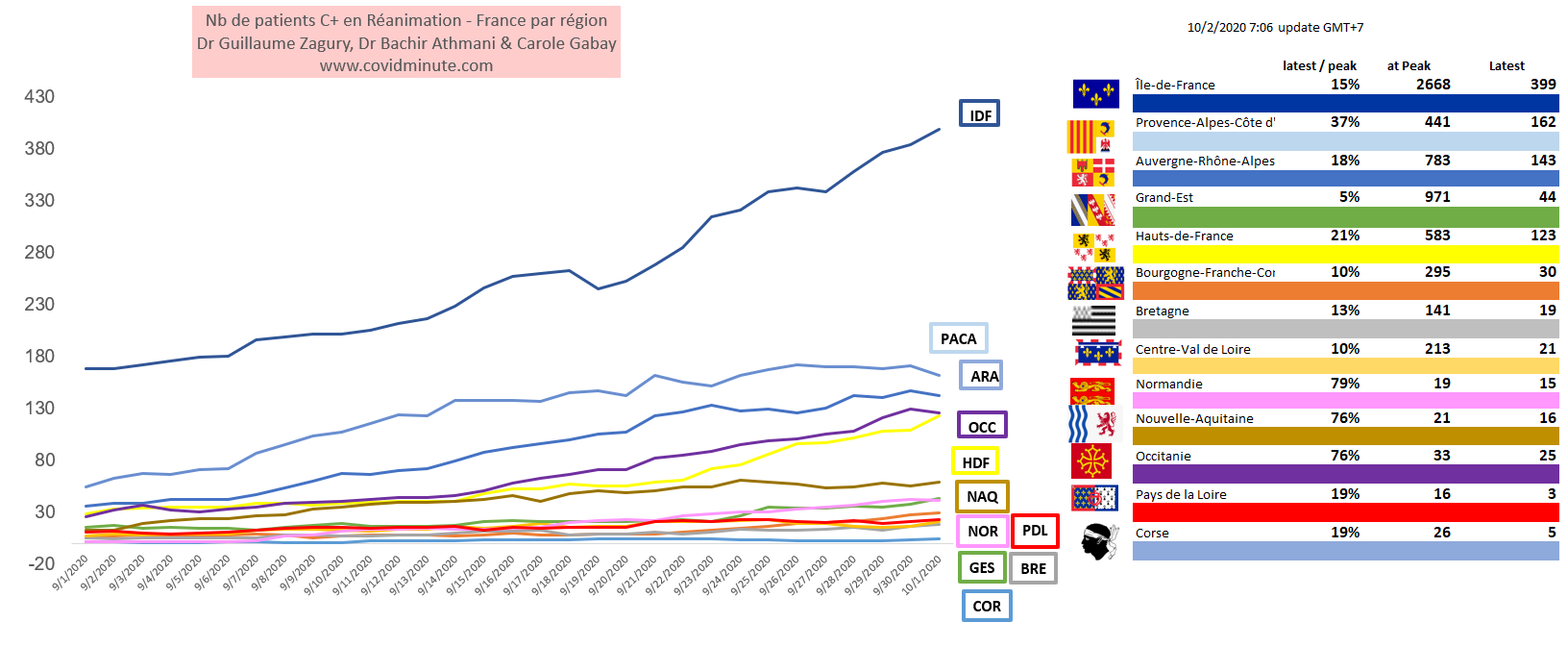
At regional level:
The system begins to be powered up in IDF, and stabilization in PACA (see appendix).
Note the physical and moral fatigue of many caregivers, with the idea of ”putting it back”, while already having “the film in mind”: the number of work stoppages in our Public Hospitals (already in just-in-time before Covid ) will be a good indicator to watch.
⚠️ To go further
1/ Chronological Vision (Time)
2 & 3/ Regional Barometer & DOM TOM
🇪🇺 Europe : “Barometer per country”
A North South gradient observed
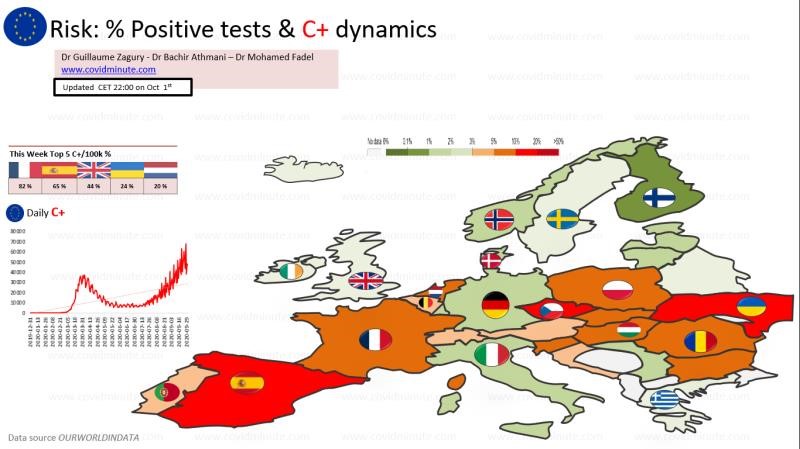
In terms of “homogeneous” comparisons, let’s not forget that we must reason at 4 levels: local (department) – regional – national – European
8 countries are currently “sensitive” in Europe: Spain and France in the south and some countries in the East (Romania, Czech Republic, Ukraine,…), but also Belgium and Holland are to be watched
⚠️ To go further
World : “World pandemy”
Time : A 5 kinetic viral phase
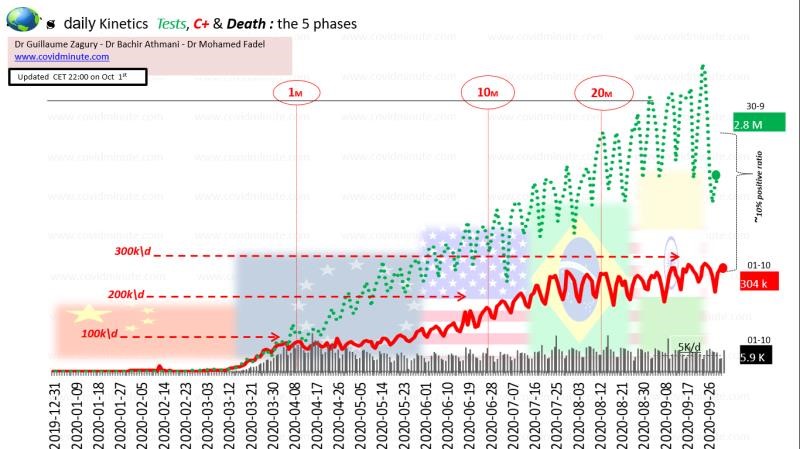
Have the few key figures in mind: 5k deaths / day and +/- 300k new officially declared C + / day (beware of everything that is “test dependent” in terms of measurement and interpretation).
Difficulty anticipating the kinetics of this pathology in the short to medium term …
Space: India takes over from the Americas (improving trend to be confirmed)
For the USA and Brazil, it seems that the situation is improving but very gradually (still nearly 1000 deaths yesterday)….
⚠️To go further:
6/ Kinetic deaths for major epidemic countries
« Out of the box » (weekly zoom)
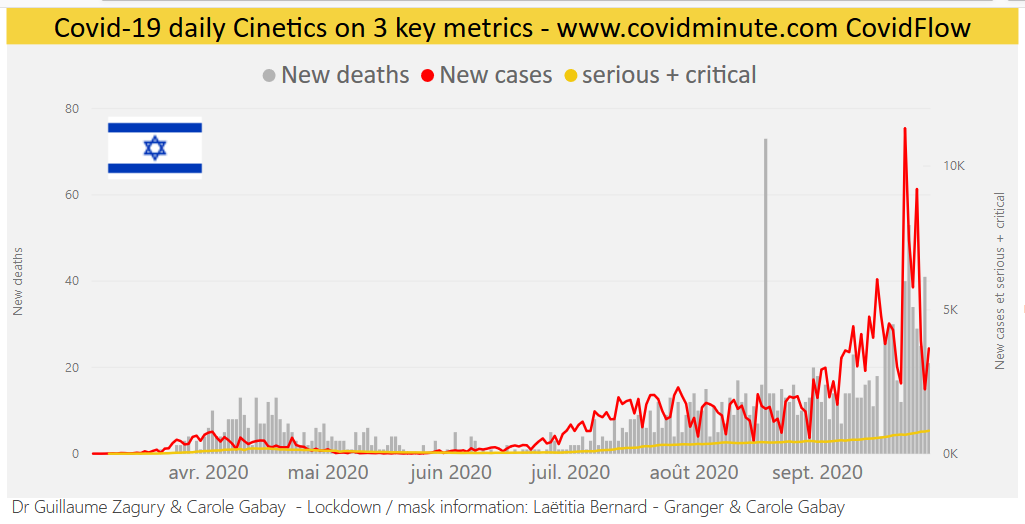
Was the Israeli Government right to close the country for 3 weeks… just before the 3 religious holidays?
As the deaths (75%> 75 years) are generally delayed on +/- 2 weeks, compared to the diagnoses, it is still difficult to pronounce in order to see the impact of the measures….
And it will be difficult to say, because this requires measuring the overall impact of health gains (diagnostic and therapeutic delays, induced mental pathologies with its risk of suicides, etc.), not to mention the economic and politico-social consequences ( division of the country…).
If we go further, we end up with a technocratic reasoning evaluating the price of a year of life gained in a senior, versus a figure with variable geometry (health + economic + social). As we say at HEC: “If You cant measure it, you cant manage it”.
To be followed weekly …
In the age of the “information highways”, relayed by social networks, our goal is thus to “return to the fundamentals”: to bring out daily 5-6 “strong signals”, factual rather than emotional, in the “noise” surrounding, and thus reassure the greatest number, in the face of a pandemic always evolutionary.
« All success is collective and so thank you to our teams (Dr. Bachir Athmani, Carole Gabay, Richard Coffre,…), as well as to our patrons, and of course to the Paul Benetot Foundation/Matmut Group.
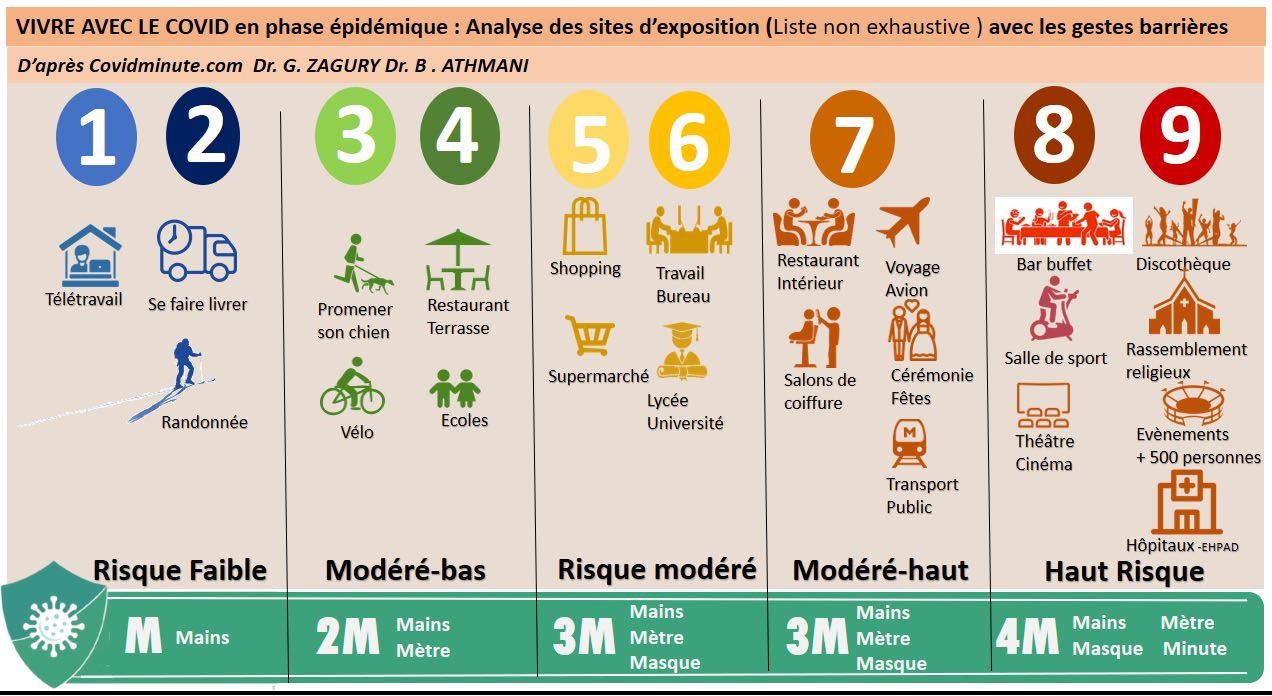
“Live with” while protecting the most vulnerable with a “citizen” attitude
- 3M for the general population (70%)
- 4M for populations at risk and the most exposed (30%)
- 4M for places at risk of exposure (case by case and common sense: visiting a church alone is not at risk, conversely, risk if a crowded place and “proximity” rituals).
See you tomorrow
Dr Guillaume Zagury
International Public Health Specialist
HEC
In China for 20 years