We know that many journalists and decision-makers (“crisis cells”, ministries, …) read this analysis “served at breakfast”, and we are delighted. We just ask you, when you use our ideas or illustrations, to have the courtesy to quote us.
Doctor Guillaume Zagury, based in Shanghai, specialist in international public health and in health innovations, comments for the Community day by day the evolution of the epidemic for more than three months, and delivers in preview the elements of understanding on its “country & region analysis” and foreseeable consequences (experiences of SARS in 2003 and of Covid-19 in China).
A whole remarkable multidisciplinary volunteer team allows the realization of this analysis which is factual and objective (moreover, do not hesitate to join us: mail below): “all success is collective”.
Beyond the voluntary skills, this project was made possible by the support of our patrons with a civic vision: the Paul Bennetot Foundation (Matmut Foundation under the aegis of the Fondation de l’Avenir), B Square, Tag Advisory , Daxue Consulting, as well as various fellow travelers (Jérôme, Dr Benoît Rossignol, Gilles Langourieux, …)
All our illustrations created for almost 100 days will soon be available on our site and you can download a large part of them. (www.covidminute.com).

I. COVID “360 * MINUTE”: 2 graphs and 2 maps (=> 80% of the information)
1. France – Time vision: we are following Italy 10 days later.
Comparative chronological evolution of resuscitation cases France / Italy
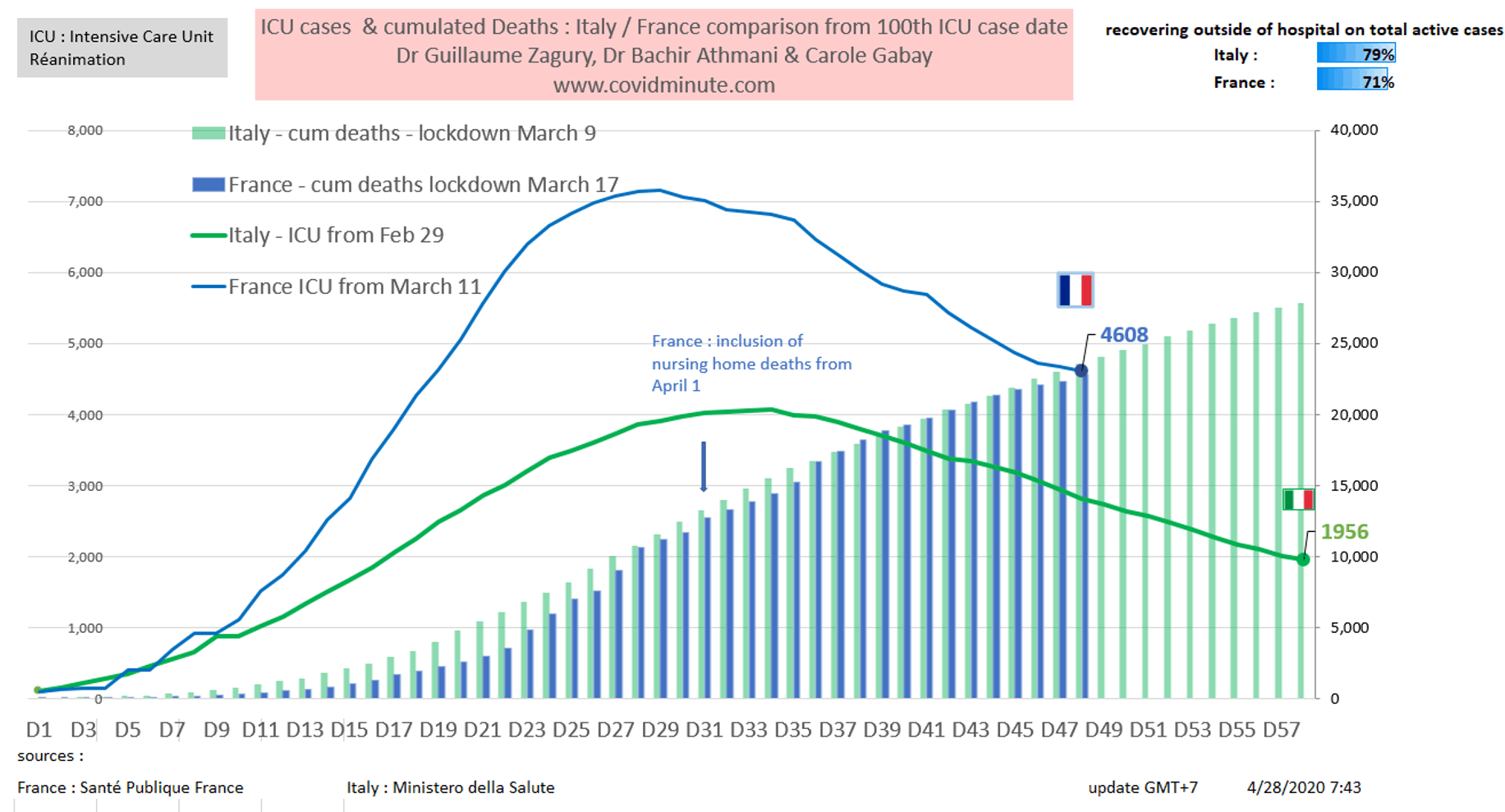
France Italy comparison from 100th case in ICU : ICU occupation and cumulated deaths
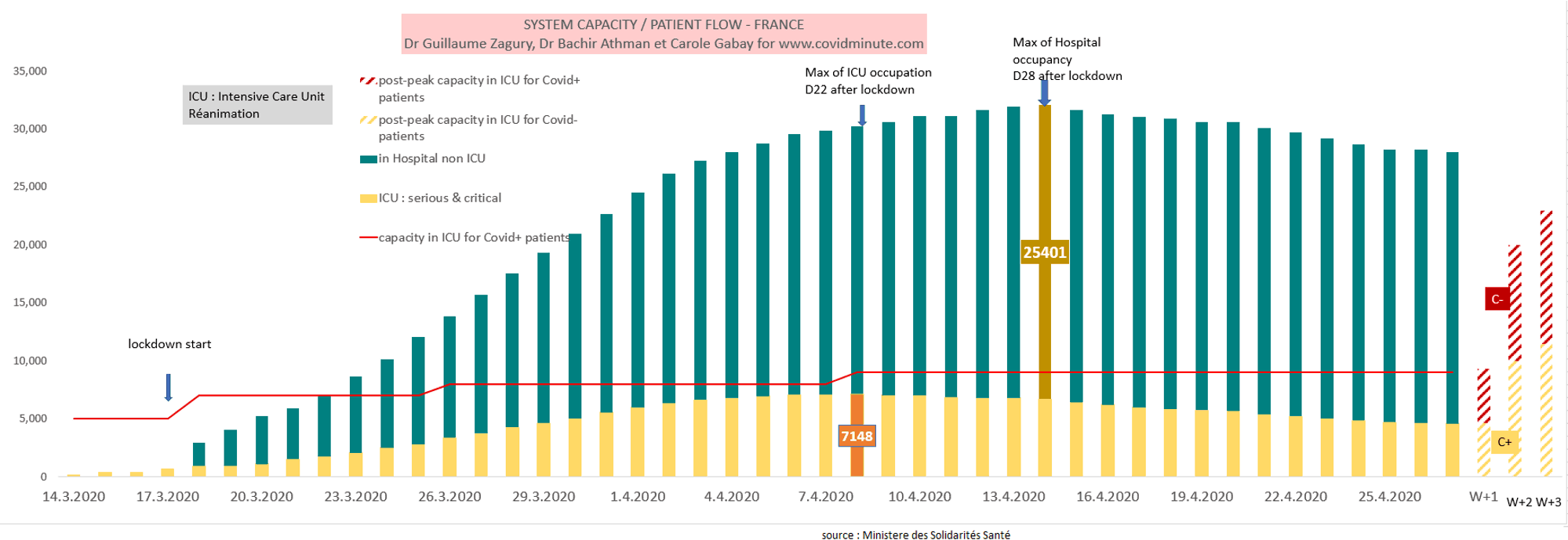
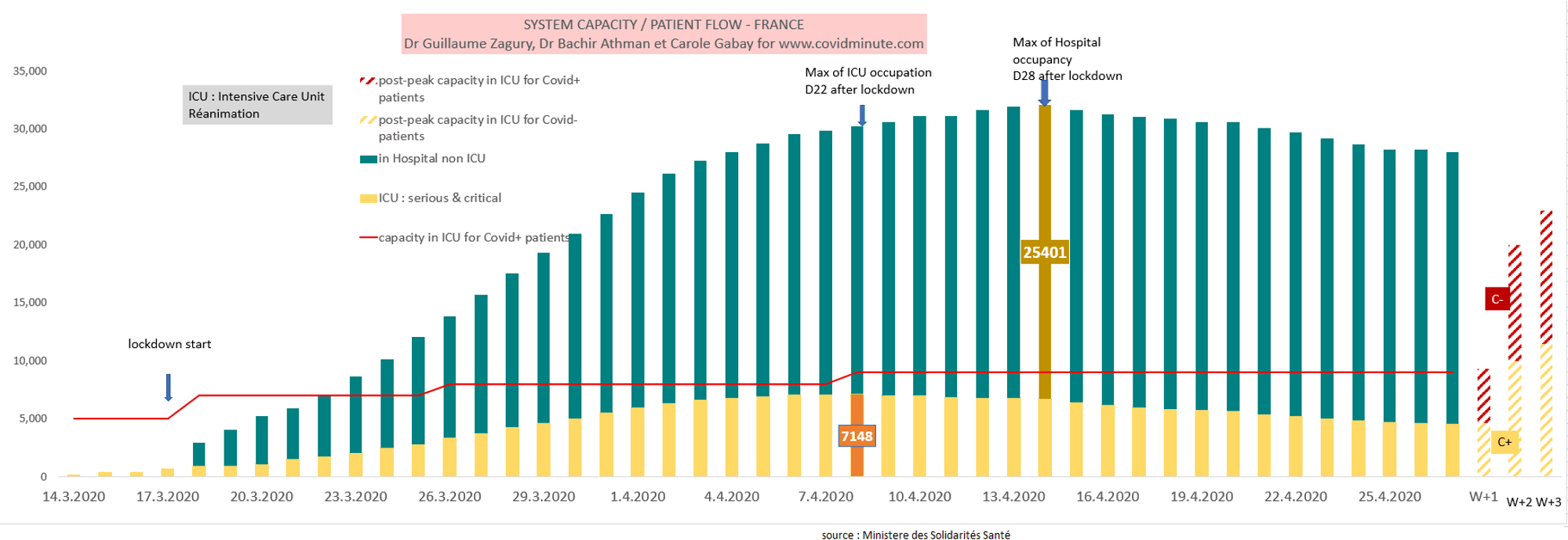
2.France – Forecast: Reanimation (the challenge) & Hospitalizations
Post-containment projection, based on 3 elements:
- historical model: peak resuscitation C (+) at S2 (7,148 beds on April 7) and peak hospitalization at S3 (25,000 beds occupied on April 14) of confinement.
- the average incubation period (1 week or impact from May 18)
- Influx of C (-) patients who decompensate soon after 2 months of poor medical care
We maintain the suggestion of the CovidMinute team, of a Covid center (+) with 1000 beds (Val de Grace or Hotel Dieu for example) for the Ile de France, which we have supported for more than 3 weeks and which has no void doubt will be taken up by the media and decision-makers. This mapping is for the rational aspect of this statement.
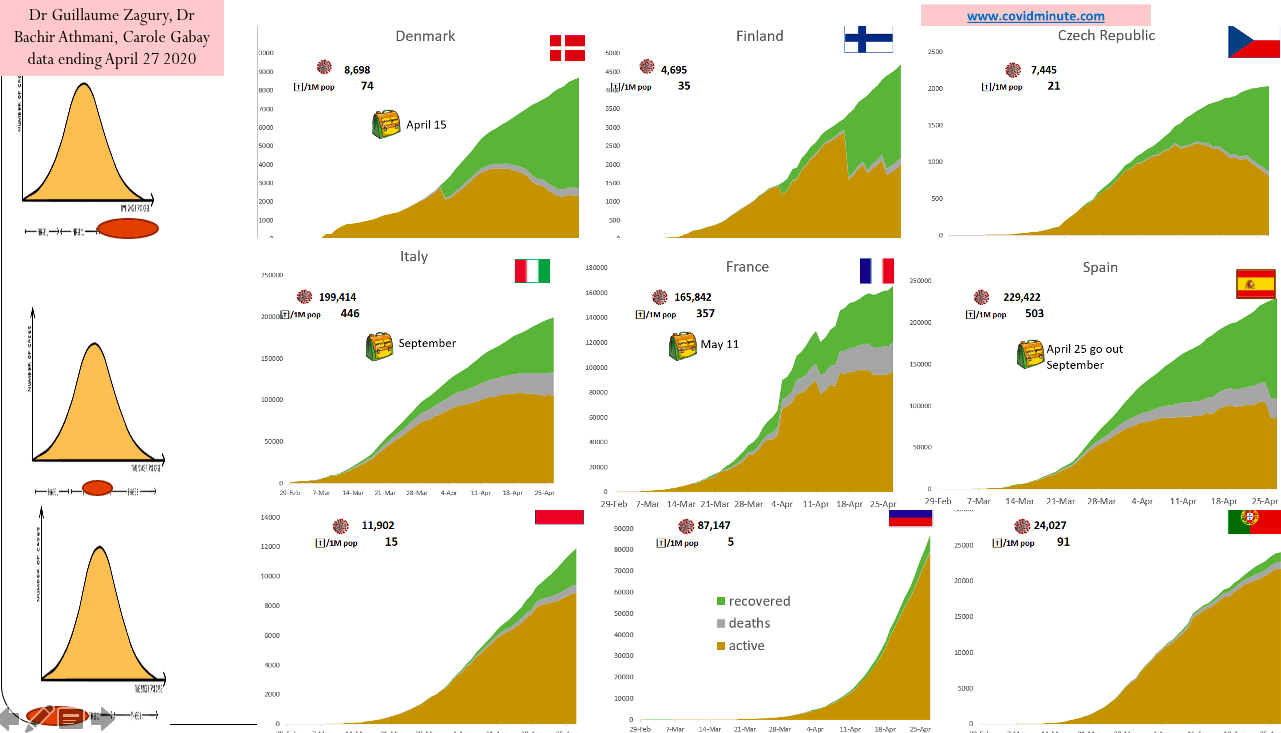
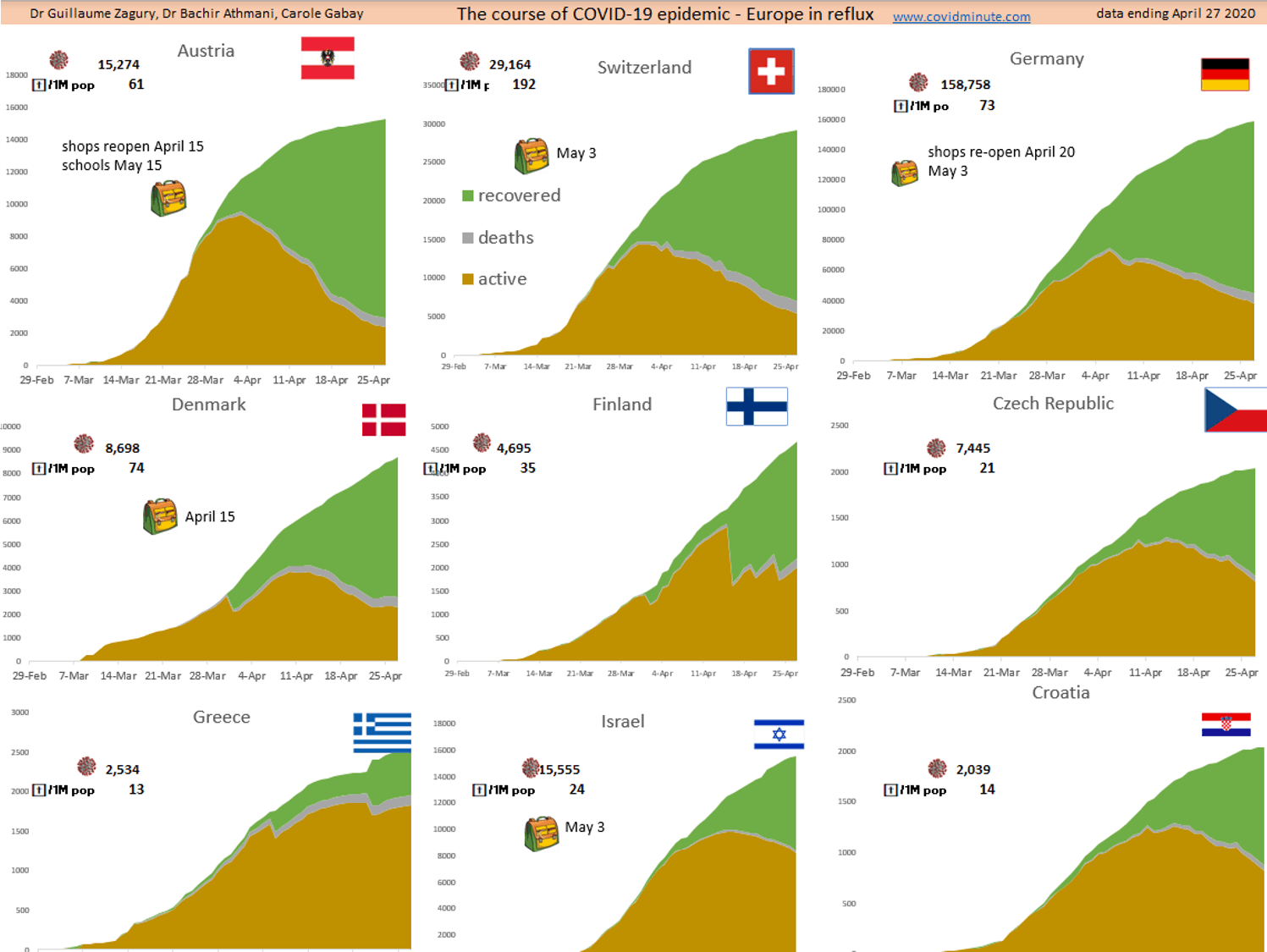
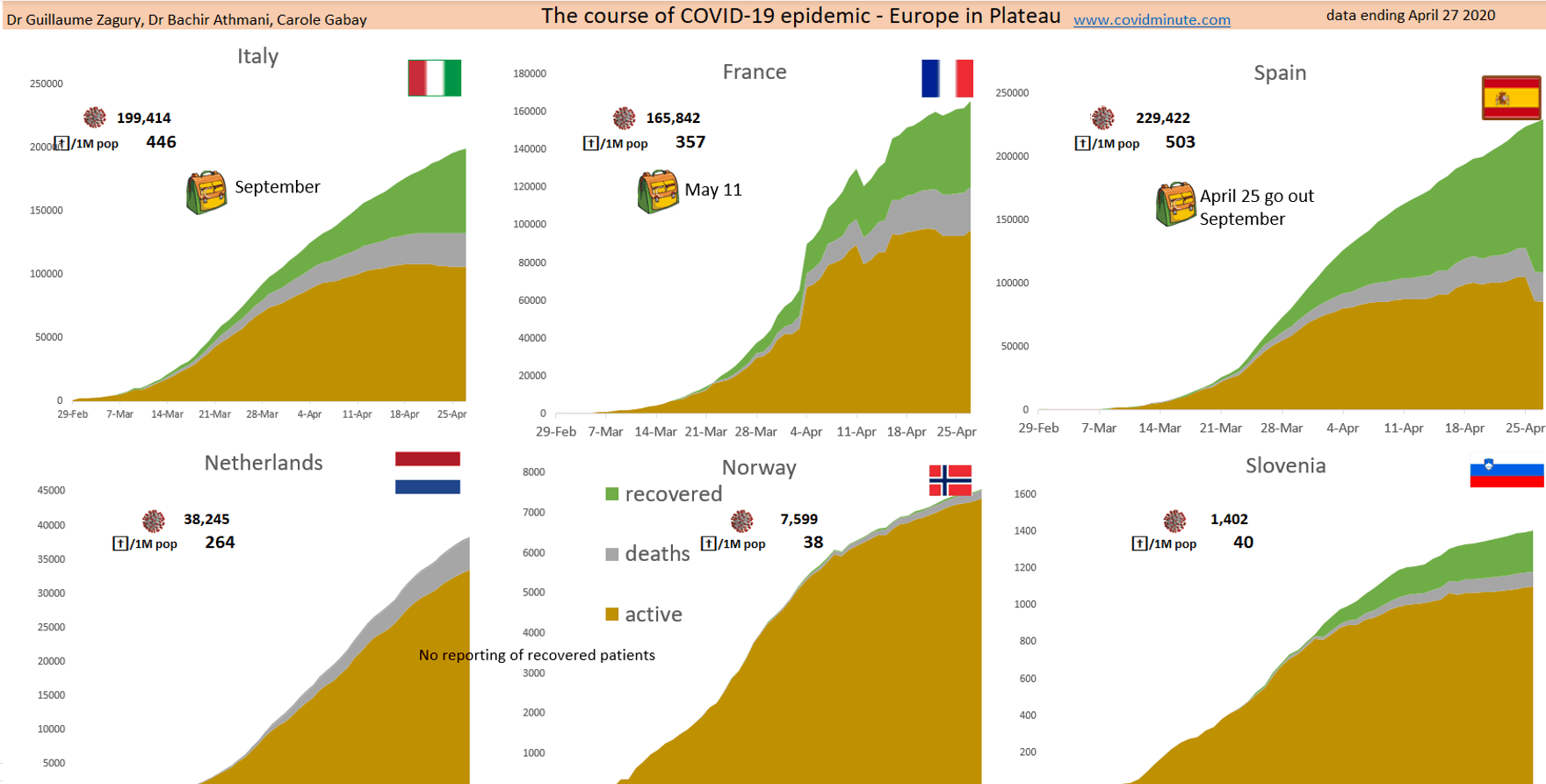
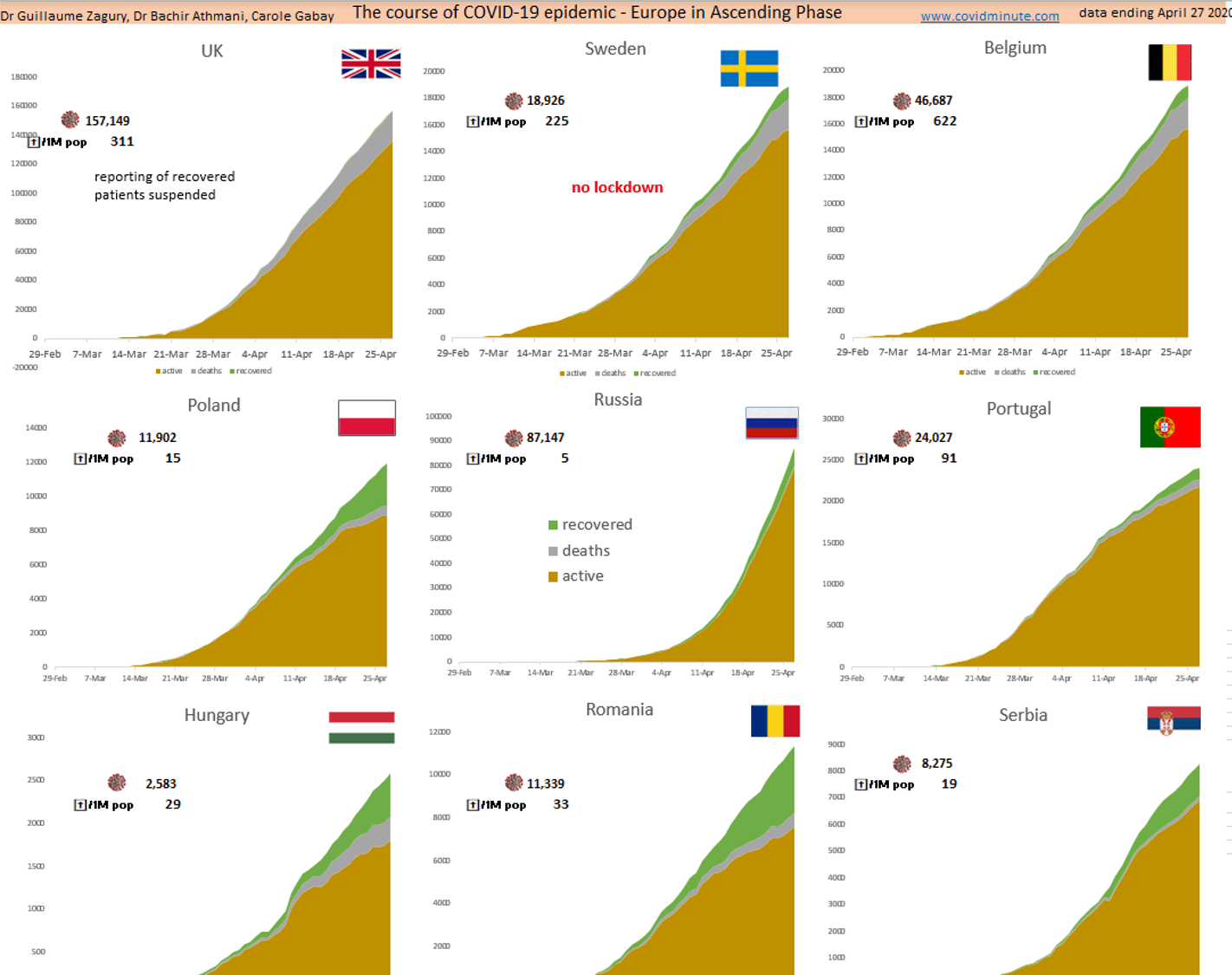
3.Europe at 3 speeds: peak – plateau – epidemic phase
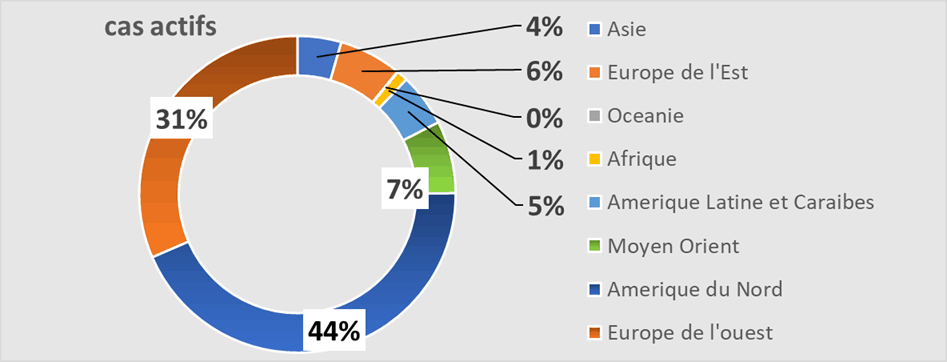
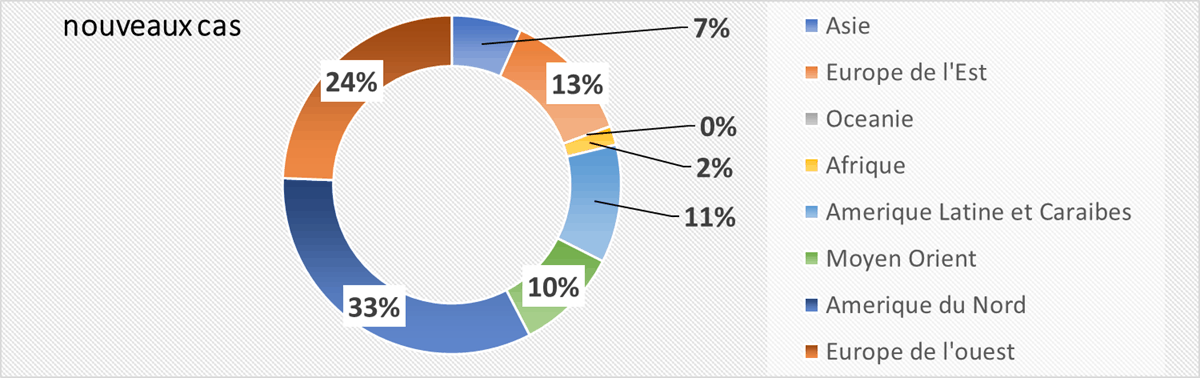
4.Worldwide
Half of the active cases declared in the Americas, a third in Europe, 10% in the Middle East.

II. 360 ° analysis (20 minutes): D42
A.Chloroquine: not enough to make a new “Dreyfus Affair”, but our team is positioning itself
A.1 Historically: a molecule known for 70 years
It is a drug known for more than 50 years (malaria and immune pathologies such as lupus or rheumatoid arthritis) and consequently no longer need to carry out lengthy studies on the market (kinetics, animal toxicity, side effects on humans ,…)
A.2 At the fundamental level, a double action:
- Anti-viral: for several years its action in vitro and in vivo has been demonstrated (clinical studies are underway within the framework of Covid).
- Immuno Modulator: however we know that within the framework of Covid, there is generally towards S1 a “storm of citokines” which makes compensate the patients. It is this action which justifies the use of this molecule for certain lupus patients or presenting a rheumatoid arthritis. Besides, an APHP team, has just produced encouraging results for this type of molecule (Tocilizumab)
A.3 At the clinical level
If its effectiveness is currently being discussed in a classic “expert against expert” debate, 2 objective elements in favor of its interest
A.3.1 The Chinese are the most experienced / Covid treatment (more than 3 months)
We know that they use it for C (+) cases, even asymptomatic (recent case that I followed in Shanghai), and that they reported very few side effects for short treatments (5-8 days) and under medical supervision.
A.3.2 The Chinese government, is currently putting “pressure”
On the manufacturers of hydroxychloroquine to produce to the maximum of their capacities. We know how much the Chinese are pragmatic (profit / risk ratio) and well informed. This was aimed primarily at health, to anticipate a possible second wave, as shown by the recent “lock down” of the city of Harbin (Russian border) 5 days ago, with 386 imported cases and 110 cases in local contamination since 1 March 1.
A.4 “Geopathology”: its widespread use in certain countries
- Maghreb countries: clinicians in their recent statements, seem very satisfied in terms of risk / benefit of systematic use at an early stage of the pathology of this molecule (combined with other very rigorous measures like in Morocco), although on medical supervision and for a short duration.
- Countries with a high prevalence of malaria (and therefore chloroquine): if a priori, the pathology has not “exploded” (see resuscitation, …) in certain high-risk tropical countries (Africa, India ,. ..), various reasons could explain it: lack of tests, “temperature-humidity” effect, young age of the populations, chloroquine impregnation, …
A.5 In total, given these 6 elements, and seen from the outside, our team of clinicians suggest:
- Taking into account the risk / benefit of the molecule, of a debate of experts not settled at the current time, of a possibility of short treatment at an early stage and in a medical environment, which it is necessary to: luck to the product ”.
- At the same time, “contradictory” and multicentric clinical studies must continue to be fixed with certainty.
- At the same time, a retrospective study (this goes quickly and is inexpensive) in Europe on Lupus patients on treatment with chloroquine (it is not the majority but we can find some!), And compare them to a control group (age , gender,…).
B. The memo-technical
Means at the service of Public Health (prevention: the only current therapeutic weapon) and of citizen action (“I protect myself to protect others”): the “Stop Infection” shield adapts to the 3 levels of risks (with each level of risk, its level of response).

B.1 ⅔ of the population
“3M” – Mask-Main- Meter (initially Sick when we did not know the fact that about 50% of C + are asymptomatic) _
B.2 ⅓ of the population
Caregivers (around 2 million including 1 million doctors and nurses on the front line) and people at risk (around 18 million: 65+ years old & underlying pathology) add the temporal aspect: memo => Minute
B.3 For the rare professionals working at a higher risk level (laboratory handling the virus)
Add the strict preventive aspect: memo => Manometer (pressurized combination, ….)
B.4 For decision-makers
Our “3M 3T” matrix, which enables the strategy to be rolled out into 6 essential concrete actions from our CovidScore table, published 3 weeks ago: Individual concrete measures (“barrier gestures) and collective measures:
- Masks: stock
- Hands: stock of hydro-alcoholic gel
- Meter: social distance (meeting…)
- Test: stock (around 700,000 / week)
- Tracing: application allowing to go back to the contact subjects
- Temporary: isolation of Covid patients (+) or contacts in suitable structures (4H): Hospital-Hotel-Accommodation center (stadium, ..) – Home, …… until recovery or quarantine period ( 12-14 days)
C. France J41: 2 important elements for deconfinement
C.1 Hospitalizations: downward trend (between 500 and 1000 cases / day at national level) and this in all regions:
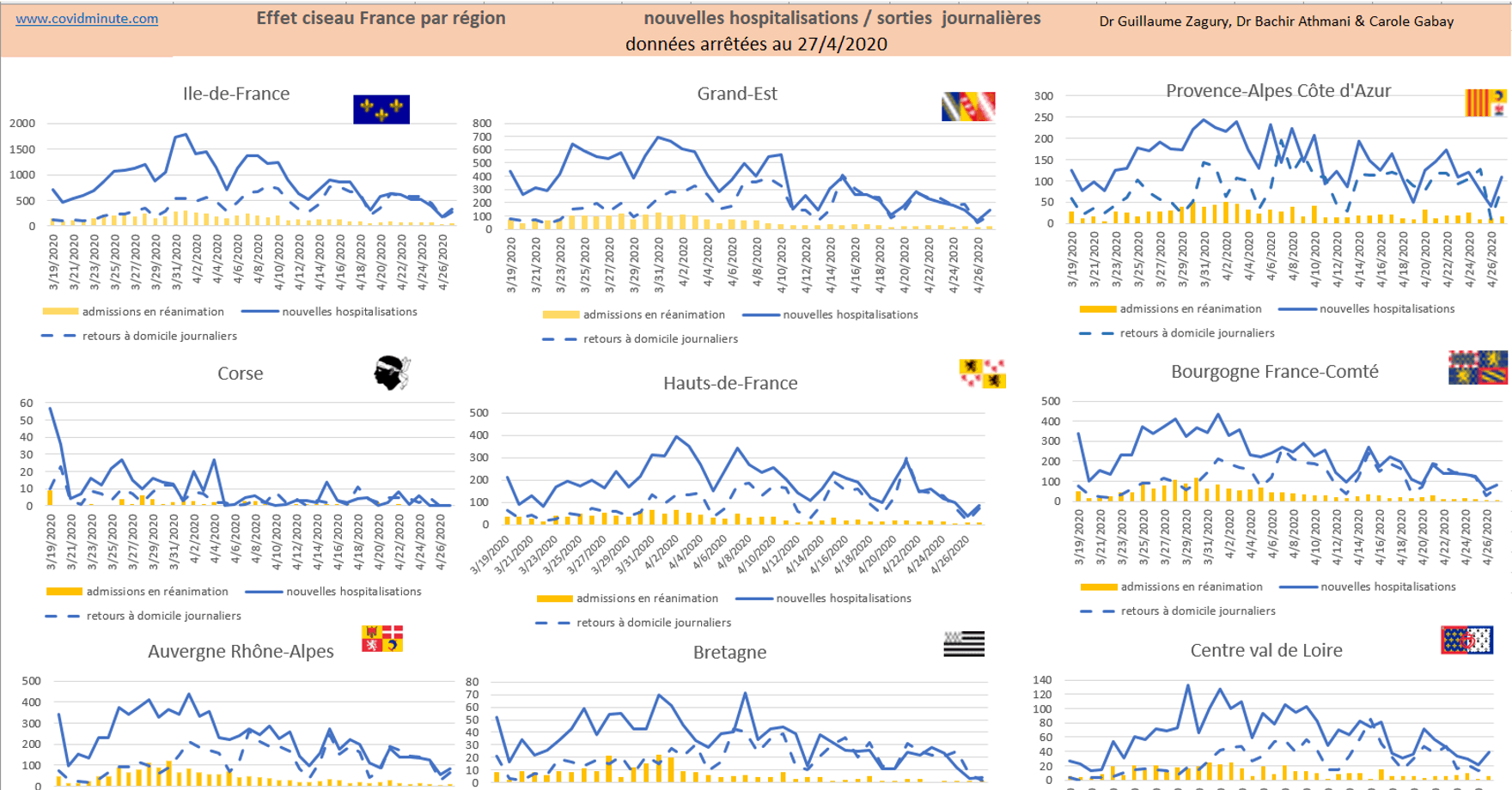
C.2 Resuscitation: decrease in C (+) -74 cases yesterday, in all regions.
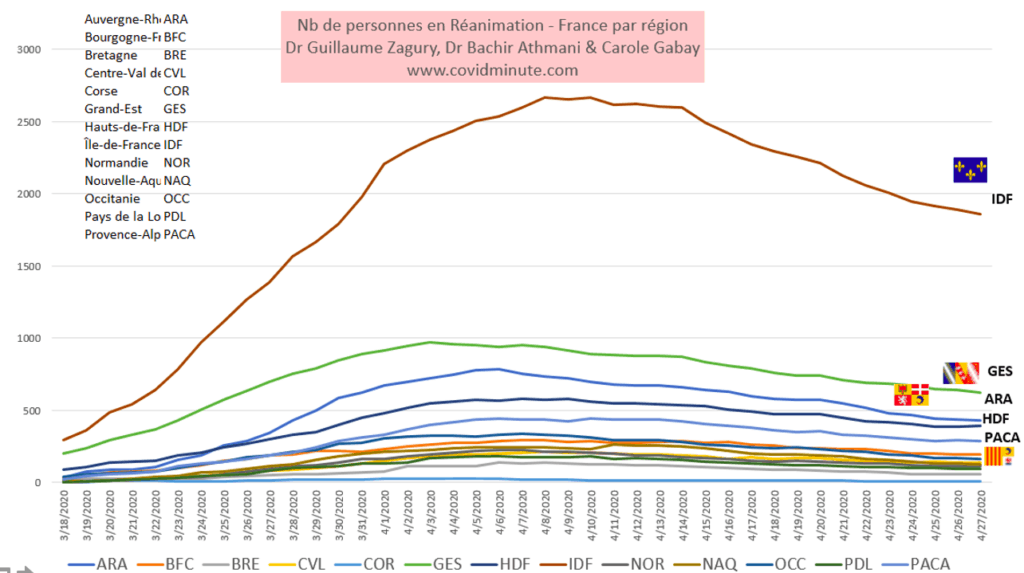
Occupancy of beds in ICU by region of France
With 4600 resuscitation beds occupied by the Covid (+), we are still in pre-saturation (more than 85% of our capacities), because the Covid (-) cases are starting to flow.
- Also, the admission criteria, drastic, 15 days ago (intubate-ventilated patient), have been relaxed for Covid (+) and there are fewer intubate entrants than previously.
- Hence our persistence in the establishment of a structure of 500-1000 beds in Paris, to manage the C (+), in order to release the C (-) requiring care to join the care structures (we do not of medical acts by telemedicine!).
- Our team, very often several weeks ahead of the events, persists in this orientation and as we are read in the Ministeres and crisis cells, … I think that the acts will follow either pro actively, or under the epidemiological constraint .
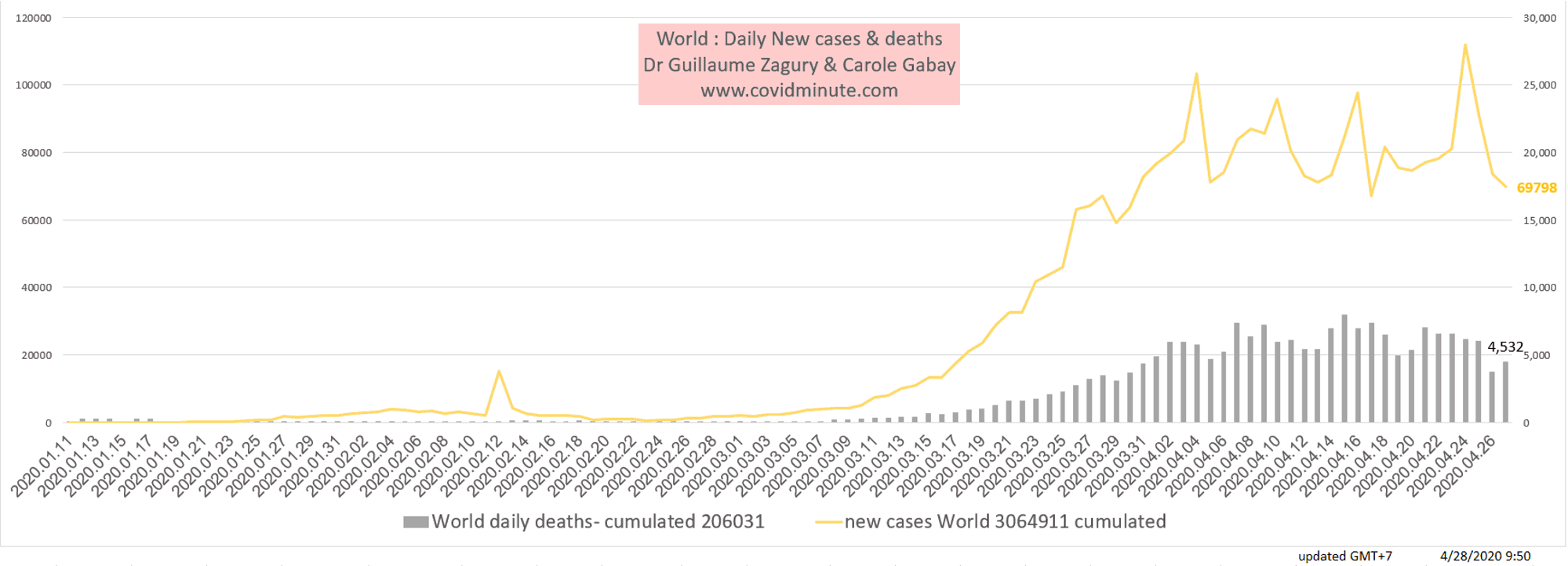
D. World: 3 billion confines, 3 million historical cases, and soon 300 k deaths in 3 months (mnemonic to fix the key figures).
With the contribution of Dr Bachir Athmani and Stéphane, companions from the start, whom I thank again for their unfailing support.
Beware of certain figures (number of cases, deaths, etc.) which are extremely questionable as they vary from one country to another (example: availability of tests), with measurement bias and therefore major under-reporting in certain countries. .
D.1 Prevalence: 2 million cases currently under observation
D.1.1 Geographic vision:

D.1.2 Continent: Europe 1/3 of cases and 2/3 of deaths to date
D.1.3 Top 10 countries
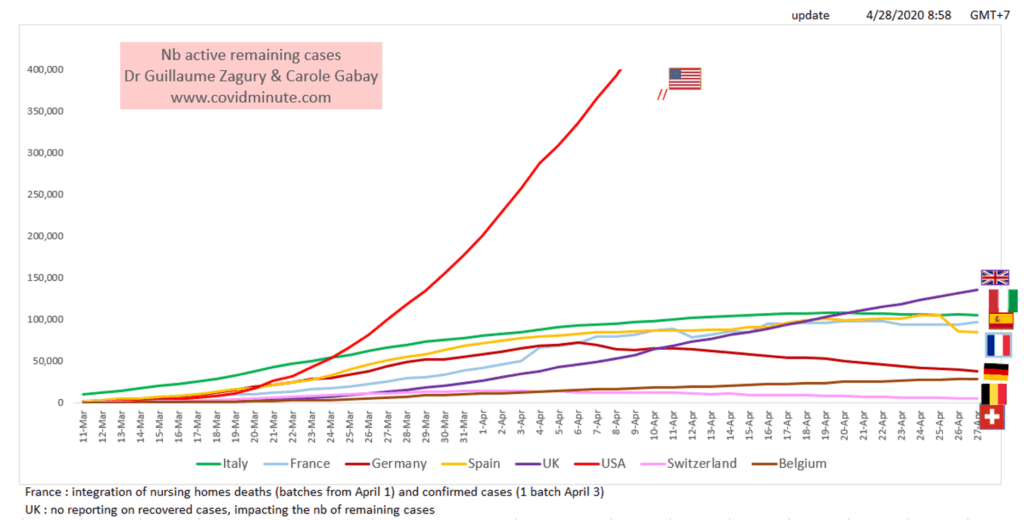
Daily trend by country in nb of active cases – Germany reflux is showing well
D.2 Incidence: the epidemic has slowed down all over Europe
Dynamic vision
By country
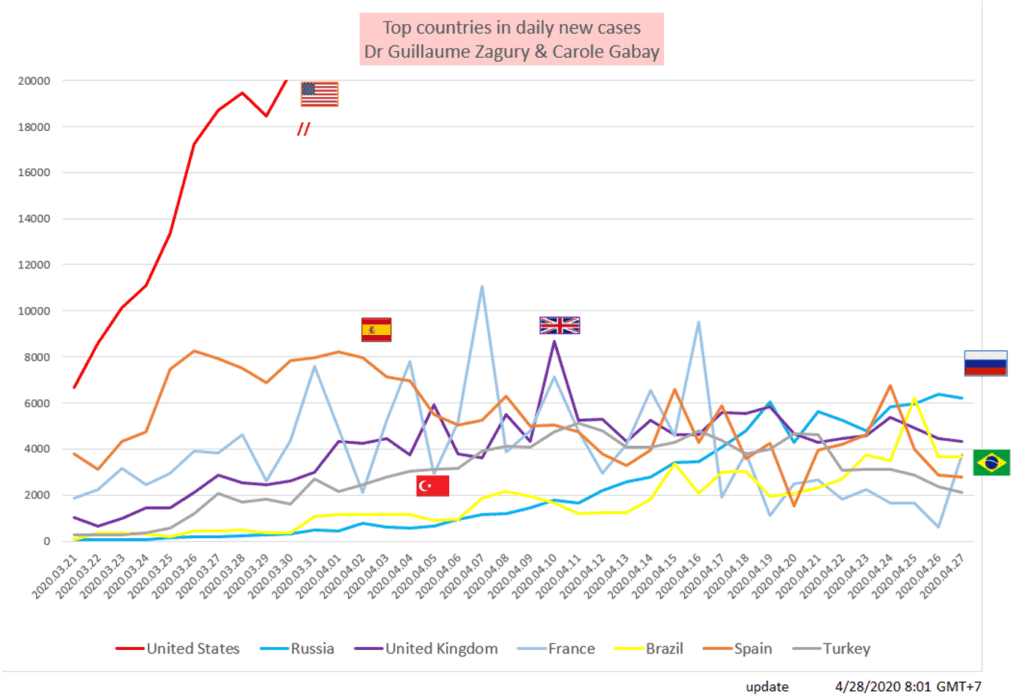
Today’s Top 7 countries in daily new cases, daily trend
By Continent:
D.3 A Europe of deconfinement
At 3 speeds depending on the epidemiological situation (Austria, Czech Republic, Portugal, …) or their health policy (Sweden: no confinement): epidemiological point.
E. TOMORROW
Update on the USA
Keep in mind the “3M reflex” (Hands-Masks-Meter) to protect yourself… but above all to protect the most vulnerable.
Trust and solidarity for this collective fight
Dr Guillaume ZAGURY
“All success is collective”, thanks to:
the entire “Medical” team of the “GCMN” type (Global Covid Medical Network): Dr Bachir Athmani, Dr Marc Abecassis, Dr Mohamed Fadel, Dr Ibrahim Souare, Dr Jonathan Taieb, …) which allow this project to exist,
the entire data analysis and IT team: Carole Gabay (“Data Analysis Expert”), Richard Coffre (exceptional webmaster), Flavien Palero (digital manager), Mathieu Bouquet (for his past contribution)
the entire “Communication” team (Flavien Palero, Laetitia, Marie, Alison, …): without whom this project would not have been possible.
all historical financial sponsors (Jerome, Benjamin Denis & the B Square Consulting Company, Benoit Rossignol, Arnaud Bricout & TAG Advisory and Gilles Langourieux, …) who work for “Citizen Actions”
We also thank the Paul Foundation
If you feel like a patron or a partner to finance IT development (all the others have been volunteers for 88 days!), Don’t hesitate to contact me (guillaumez888@hotmail.com).
Also, our team even if partly based in Shanghai, will be delighted to welcome you … because there is no shortage of work …!
