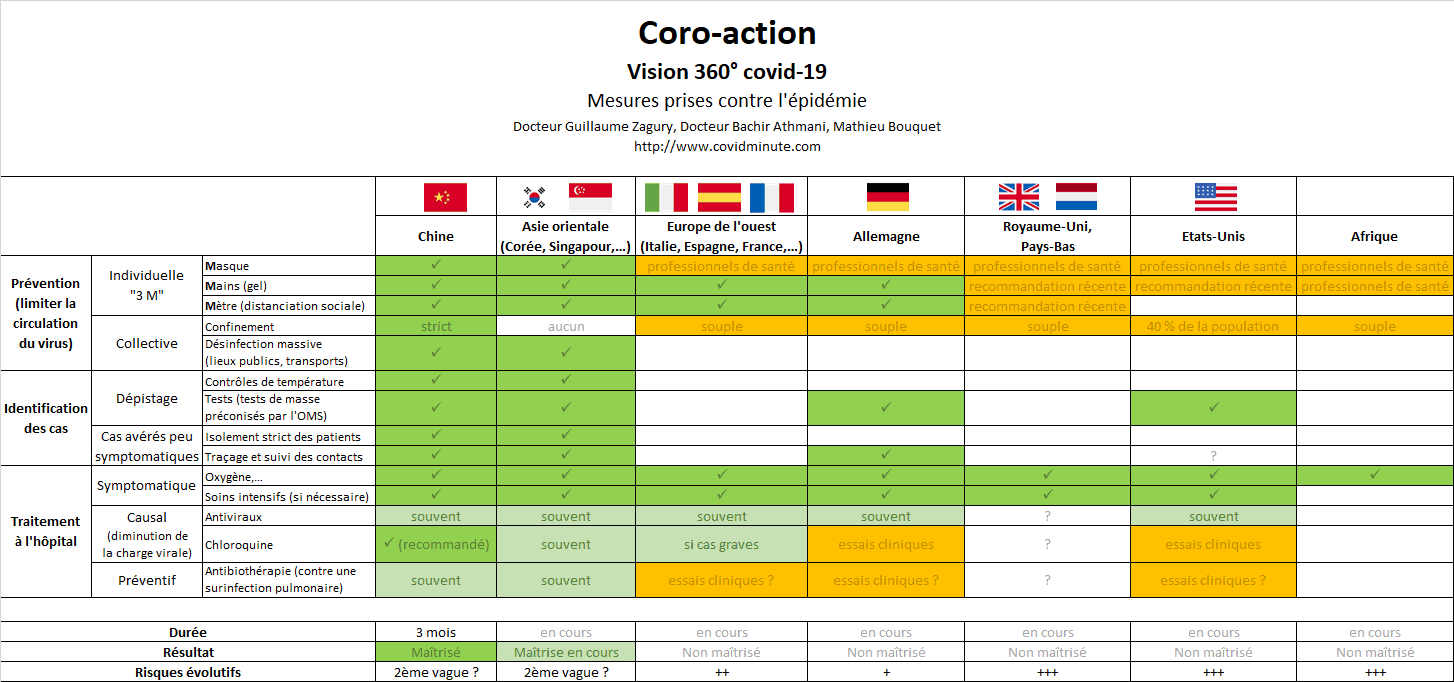
A.Measuring overall responses
Our“coroscope” indicator assesses the measures taken in a country toreduce the risk of mortality.
Thissection is produced with discussions with Dr Bachir Athmani in Parisand Mathieu Bouquetin China.
1.3 main lines of action
The response to the spread of the virus generally consists of 3 parts:
1.prevention
2.identification
3.medicalization (treatment)
Each of these 3 components is divided into several measures, which we have identified in the form of 13 main actions (lines of our table), to which we add the measures of anticipation, preparation and reaction shown by the countries.
All the actions do not have the same weight and the same effectiveness,our team therefore assigned them a weighting element evaluating theimpact of the measure, based on the results observed in the different countries affected by the epidemic, some countries Asians with more than 2 months of experience and perspective.
2. The Dashboard

This table allows to better understand that the treatment of this epidemic involves different dimensions, each with its logic:
-development of a strategy: preventive / curative and simultaneous orstep-by-step actions
-indicators to monitor: medical and social (health system)
-taking into account cultural and historical aspects: recent trauma ofSARS (2003) in Asia-Pacific (the Prime Minister of Singapore haddeclared at the time: “We will die from the economicconsequences of SARS, before dying of pathology” ).
-assessment of economic implications: multiple trade-offs to be madeat each stage
-technological (antiviral, chloroquine, vaccine, etc.) and economicreaction (purchase, storage of materials, adaptation of theproduction system, etc.)
-adaptation of policy and leadership: weight of administrativeregulation, weight of Europe in health decisions, etc.
3.Country assessment
Anote is given for each row in the table. This rating is based on themeasures taken by the various countries since the start of theepidemic.
Thebenchmark (golden standard) is based on WHO recommendations and oncountries that have so far succeeded in controlling the epidemic(mainland China, South Korea, Singapore, among others).
Followingthe evaluation of the measures adopted, each country is given anoverall rating, which changes depending on its reaction to theepidemic. We are delivering a first version of this assessment below,which will improve over time.
France(overall score of 10 out of 30, 30 corresponding to the maximumstandard) is in our eyes evolving towards a more offensive strategy,and we can only welcome it, hoping that the declarations will befollowed up fast.

B.France D13 – Massive influx of patients to the hospital for at least a week
The elements below are to be read with the reservations concerning the validity of the data (case definition, possible underestimation,etc.) already mentioned above, and keeping in mind that it is the trends that count, rather than the raw figures taken at time t .
1.Incidence: +4,611 new confirmed cases (3,809 yesterday)
We are still in the epidemic growth phase.
2.Prevalence: 29.5k active cases under observation (25.2k yesterday)
On this basis alone, the doubling time is reduced compared to yesterday(but a trend measured over only 2 days is not significant) and is between 5 and 6 days.
3.Trend (comparison with Italy): close trajectory
To date, France’s trajectory remains relatively close to that of Italy,with all the necessary precautions for this comparison, in particular on the testing strategy adopted by each country (case definition).
But as specified in 2, what is informative, is the chronological trend:
if France continues to follow the Italian model, the peak could be expected around mid-April

4.Health system
4.1.Capacity building
A huge effort is being made by the health authorities and we must congratulate them for increasing our capacity for handling difficult cases from 7,000 to 14,000 beds.
Similarly,let us highlight the 2 essential initiatives, with orders for
-masks:one billion to China (or 56 Antonov round trips) for an estimated use of 18 million units per day.
-tests:a large order in China and a request to our laboratories (human and veterinary) to advance on the development of “minute test”,which certain countries (Belgium, United States, Thailand) are in the process of putting in action.
4.2.Patient profiles
Let us remember that this pathology affects above all fragile people …but not only:
-thus, 2/3 of French intensive care patients are over 60 years old
-in Italy, three-quarters of deaths are concentrated in patients with 2 or more comorbidities (age, obesity, asthma, etc.)
-as these elements are only statistical, we sometimes have cases of young patients with no history who die (see the 16 year old girl who died in a few days at Necker hospital).

Note also the massive influx of resuscitation patients (+/- 5% of hospitalized cases) in regions with high prevalence.
4.3.Mortality
Note the dynamics of mortality rates (an indicator that is doubtful but its dynamic is a good indicator) on the rise in France, and which only reflects the difficulties encountered more and more frequently by carers. This also applies to Spain.

It should also be taken into account that the figures provided are probably highly undervalued compared to reality, since only the figures for hospital mortality are included and therefore they do not include figures outside the hospital (Ehpad, deaths without test organic produced, etc.).
5.Territorial distribution
Anew counting method is being implemented, with a significant reassessment expected of the number of cases following the authorities’ declarations. The figures by region will be provided in a more usable way for everyone in a few days.

6.When is the peak?
There are different multi-parameter computer models, but no one can exactly predict the exact date of the epidemic peak (too many parameters to consider: evolutionary trend, temperatures, impact of measures taken,etc.).
Asian indication, the case of Wuhan: following strict confinement measures, the peak was reached around D20 after the confinement measures.

If we follow the Italian model, the peak could occur in mid-April in France.
7.Analysis of current capacities in relation to flows
Testimonyal ready quoted from an emergency room colleague in the Grand Est: “I have never had this experience: we usually have 150 visits to the emergency room and at most we in tubate once a day. Today, we have received only 70 patients but we had to in tubate 10 ”.
Our system is still able to absorb the wave (while Italy does not), but probably not for long.
C.World impact: an exponential dynamic
Thanks to Stéphane, companion from the start for his participation.
Of course with all the necessary reservations about the validity of the figures (availability of tests, validity of the data, etc.), but what is essential is the trend.
1.Incidence: 66k new cases diagnosed (64k yesterday, 63k the daybefore)

This is 20 times the figures observed in China (approximately 1 / 5th of the world population) at the time of the peak in Hubei (3k per day).
2.Spatial vision: 90% of new cases are detected in the West (60% inEurope and 30% in the Americas)
2.1.By country
The United States and Spain remain in an exponential phase.
• UnitedStates 19k
• Spain8k
• Germany7k
• Italy6k
• France5k
• Iranand England 3k
• Switzerland,Netherlands, Belgium: 1 to 2k approximately
Table:evolution by country

Chart:evolution by country
2.2.By continent

D.Prevalence world – In a few days, the United States has a number of cumulative cases higher than that of China in 2 months!
1.Figures (active cases)

The doubling time is 5 days (stable).
2.Spatial vision
2.1.By country

Top6 countries:
• UnitedStates 118k (79 yesterday): ¼ of the active cases on the planet
• Italy 70k (62 yesterday)
• Spain 55k (46)
• Germany 49k (38)
• France 30k (22)
• Iran 21k (17)

2.2.By continent
Westernerscurrently represent 83% of patients diagnosed!
Virus Preventions 4 W’s:
Wear a mask, Wash your hands, Watch out for sick people, Wait for new updates from covidminute.com !
Protect yourselves, and above all protect the most vulnerable!
Dr. Guillaume ZAGURY,
Specialist in Public Health and Health Innovations
Consultant at “Health Innovations”
HEC
In China for 20 years“All success is collective”, thanks to:
– the whole “Back Up” team (Mathieu Bousquet, Carole Gabay, Flavien, Marie, Laetitia, Anne-Sophie, …), without whom this project would not have been possible.
– all the “Medical” team (Dr Bachir Athmani, Dr Ibrahim Souare, Dr Taieb, Dr Viateur …) who allow this project to exist,
– all historical financial sponsors (Jerome, Benjamin Denis & B Square, Benoit Rossignol, Arnault Bricout) who work for “Citizen Actions”
If you feel like a patron or of partners to finance IT development, don’t hesitate to contact me (guillaume@covidminute.com).
Also, even if part of the team is based in Shanghai, do not hesitate to come and join us, because there is no shortage of work :-)If you want to find more analyses and infographics, follow our account at:Know the latest updates
Powered byMedicilline