We know that many journalists and decision-makers (“crisis cells”, ministries…) read this analysis “served for breakfast”, and we welcome it. We simply ask you, when you use our ideas or illustrations, to have the courtesy to quote us..
Dr. Guillaume Zagury, based in Shanghai, a specialist in international public health and health innovations, comments for the Community on a day-to-day basis on the evolution of the epidemic for more than three months, andgives a preview of the elements of understanding on its “country and regions analysis” and predictable consequences (experiences of SARS in 2003 and Covid-19 in China).
A remarkable multidisciplinary volunteer team allows the realization of this analysis which is intended to be factual and objective (by the way, do not hesitate to join us: mail below): “everysuccess is collective”.”.
Beyond the volunteer skills, this project was made possible by the support of our citizens’ vision patrons: the Fondation Paul Bennetot (Foundation of the Matmut under the aegis of the Foundation of the Future), B Square, Tag Advisory, Daxue Consulting, as well as various companions (Jérôme, Dr. Benoît Rossignol, Gilles Langourieux… )
All our illustrations created for almost 100 days, will soon be available to you on our site and you can download a large part of them. (www.covidminute.com).

I. COVID “360 MINUTE”: graphs and maps (80% of the information)
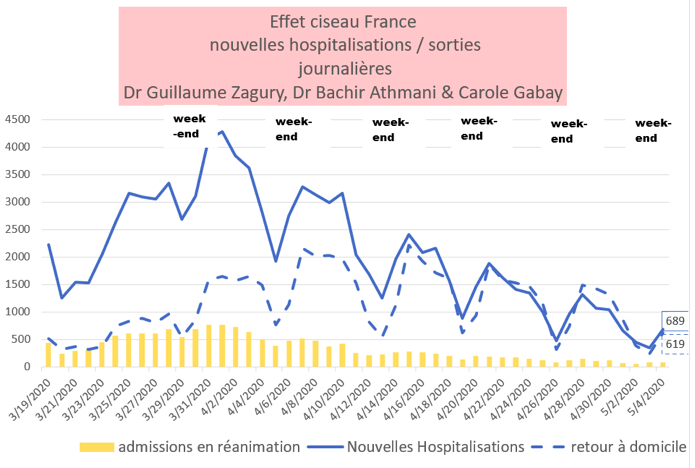
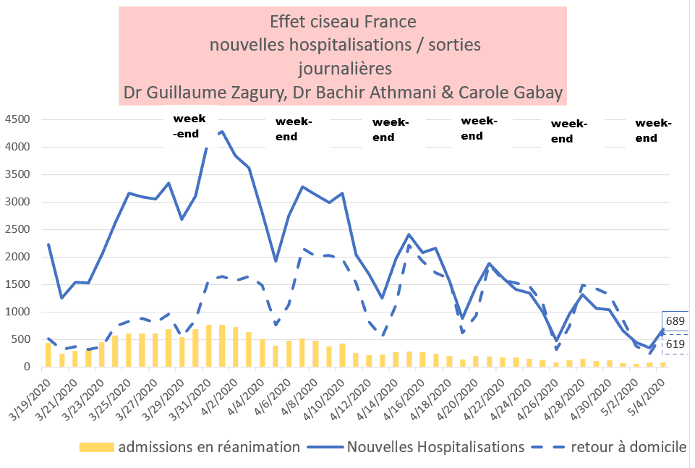
I.1 France – after 45 days of containment a favourable but slow dynamic
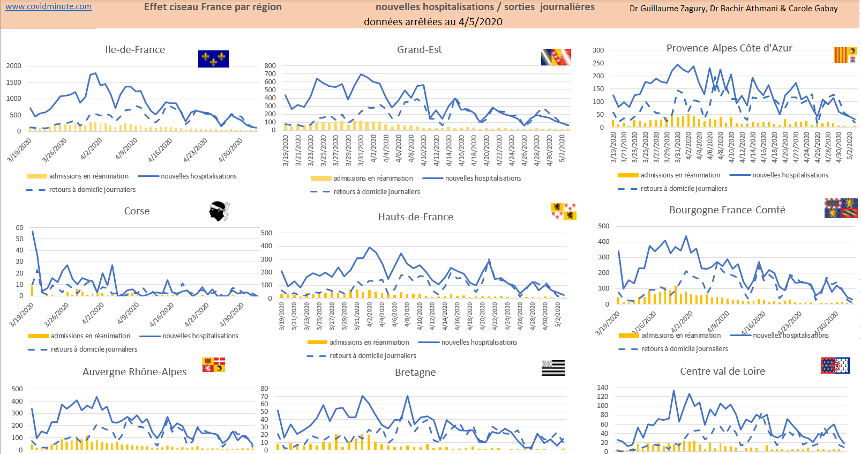
Scissor effect in progress (hospitalizations and resuscitation)
France: scissor effect in progress (Hospitalizations: more exits C- than entries C)
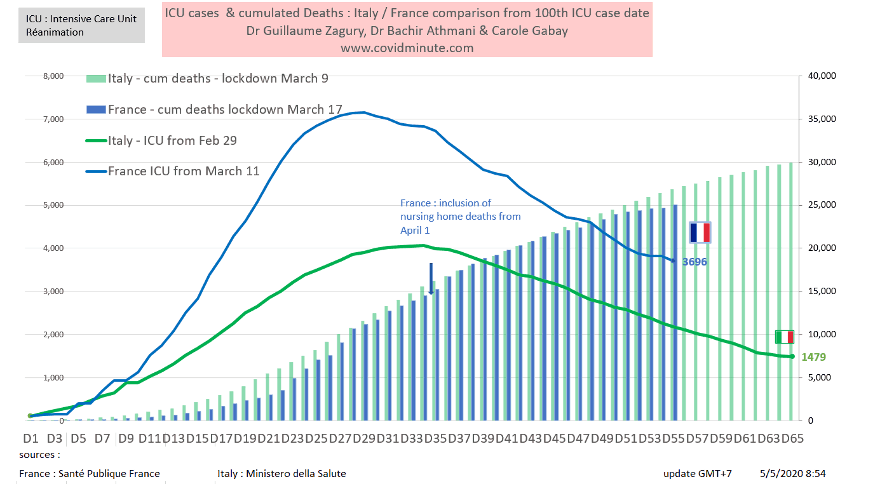
I.2 Vision time: we follow Italy with 10 days lag
Comparative chronological evolution of resuscitation cases France/Italy
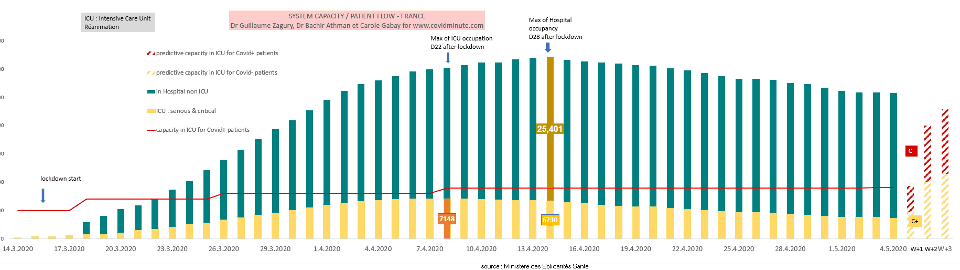
I.3 France – Forecast: resuscitation beds available (at stake from 16 May)
The Cova beds () below 4000 today (3827 versus 3878 yesterday) with a maximum capacity to date estimated at 9000 beds.
Post-disconfinement projection, based on 3 elements: historical data, incubation time (J7 with an upsurge expected around 16 May), and the influx of patients C (-) (3305 out of 7183 occupied beds)

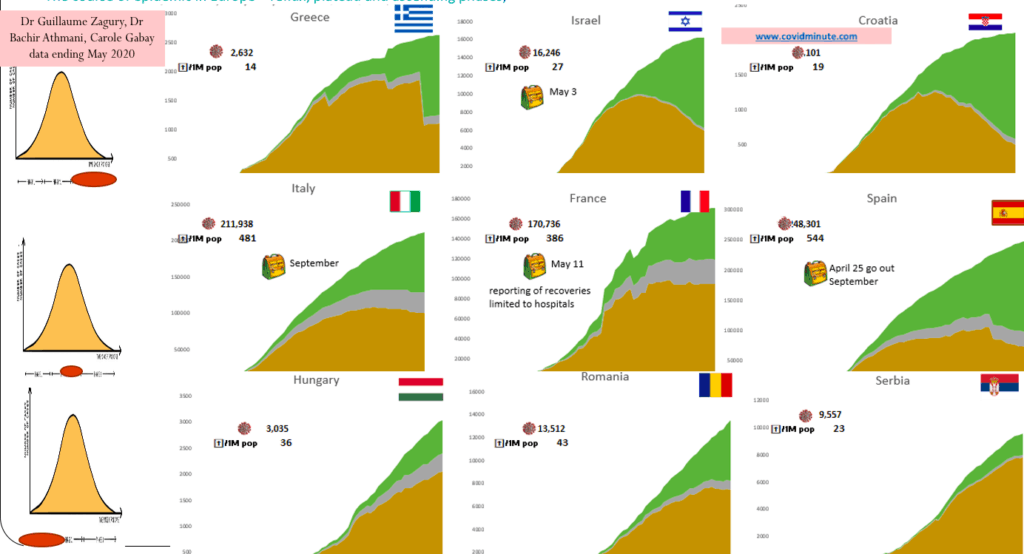
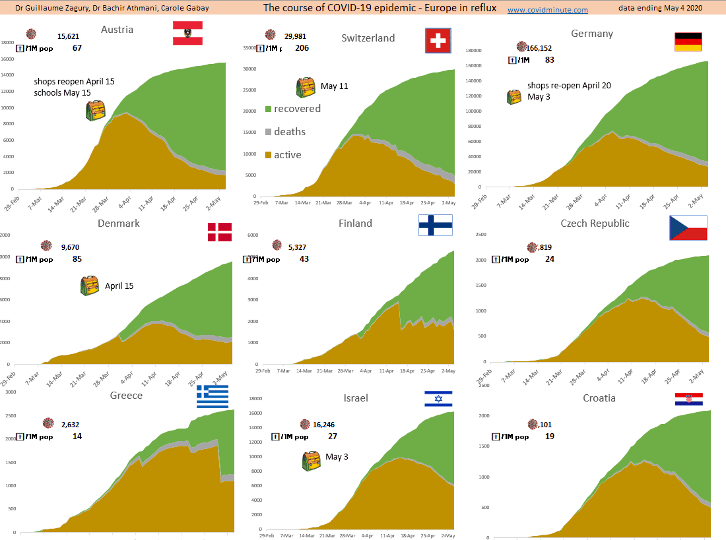
I.4 Europe: A Europe has 3 vitesses: peak passes (deconfinement) – plateau – epidemic phase

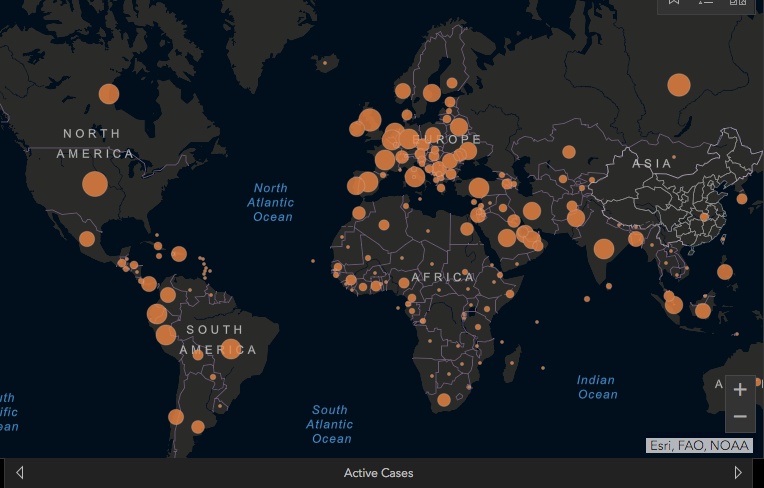
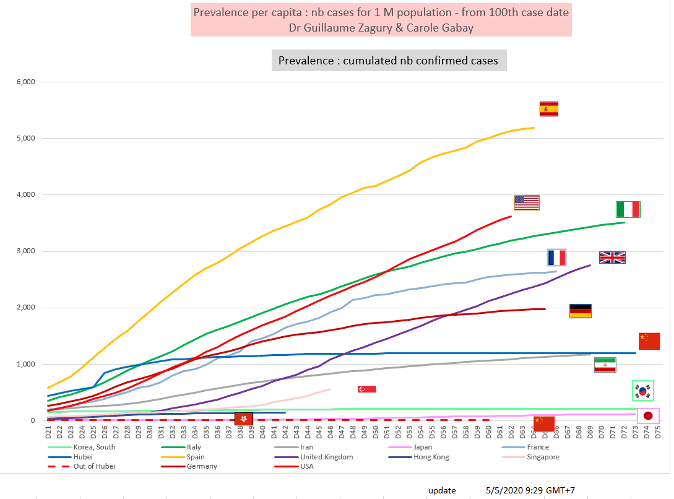
I.5Epidemic Mapping: prévalence Prevalence 70% of Existing Cases Reported in the West des cas
1.6World: Watch the BIS (Brazil-Russia-India):-Russie-Indes) :
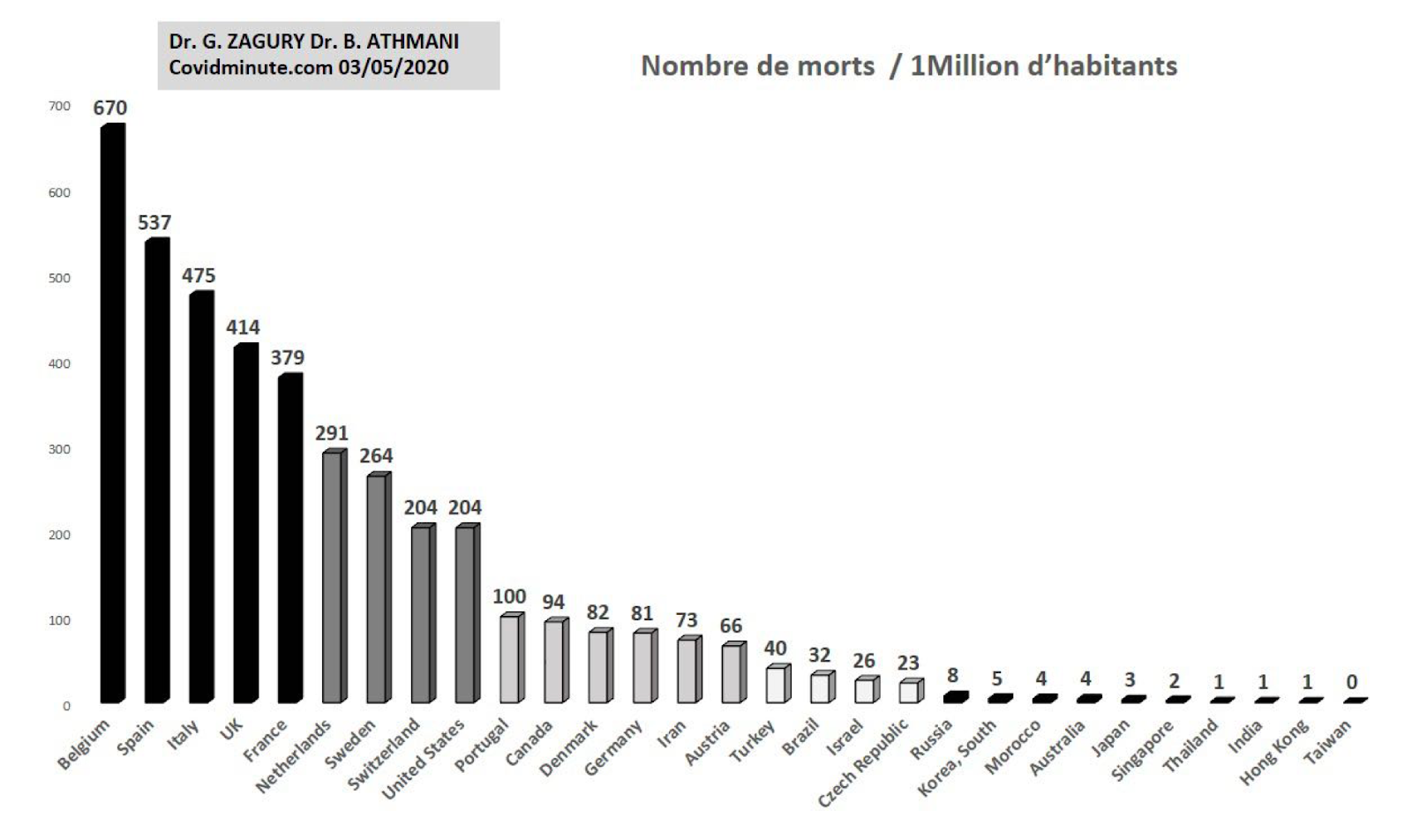
I.6 World – Outcome Indicator – Mortality / 100k individuals: 3 levels observed
Comparative international results of “country strategies”
Beware, however, of too hasty comparisons (cf Finland has low population density versus Singapore)
Indicator certainly not perfect (because depending on the tests, the density of population, the median age of the country … ) but available to assess the impact of “Country” strategies.
II. 360-degree analysis
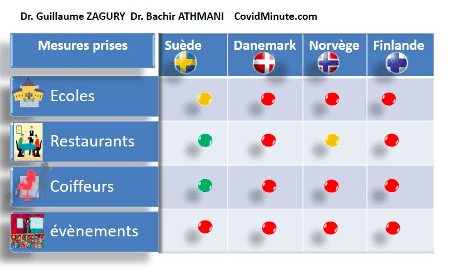
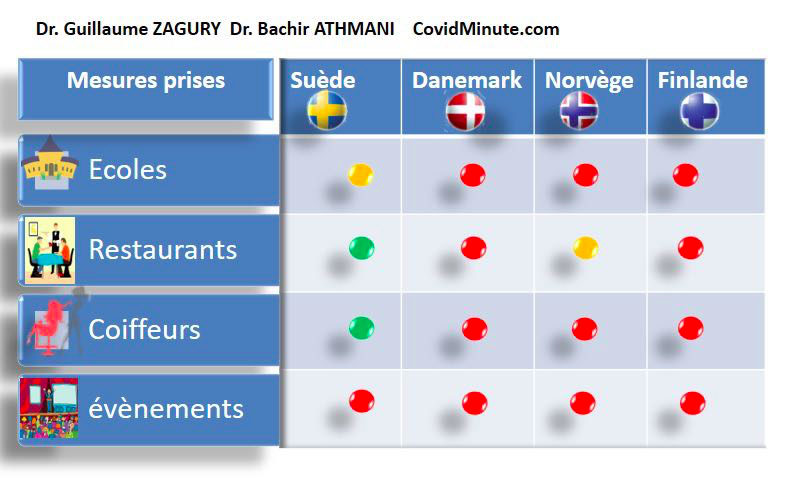
Ⅱ. A WHO congratulated Sweden on its crisis management: crise : intra-European and intra-Scandinavia panorama
I thank Dr. Bachir Athmani and Gilles Pech of Laclauze for their sharing.
Ⅱ. A.1 The Swedish Exception: choosing collective immunity against the current of Western dynamics
It should be noted that the United Kingdom had initially made this choice aswell, before backtracking arrière and returning to the principle of containment.
Sweden has been working on its own epidemiological models (particularly on the Spanish flu of 1918-1919with a decrease in life expectancy of vie de 9 years)and its own population data (without transposing Asian models).
The worst scenario for this country of 10 million inhabitants being estimated at 70,000 victims (0.7% of the population) has come into account given the average age of deaths 460.000 potential years of life lost(APVP) in 2020.One of the decision elements is also the APVs induced by a persistent economic crisis (for Sweden some economists estimating it at 10 Millions/year). éléments
Flexibility and responsiveness via constant monitoring by the government and Parliament (right of veto): System in which the health agency is independent of the government and consults medical and non-medical experts (economists, etc.)
Population support (over 65%)
Ⅱ. A.2 Our previous “Crash Test” (over a month) was titled: “SwedishRussian Roulette” Suédoise”
The CovidScore had evaluated them with a low score (class in the red où zone) as: no closure of schools, gathering allowed upto 50 people, absence of mask, absence of isolation of patients C ()…
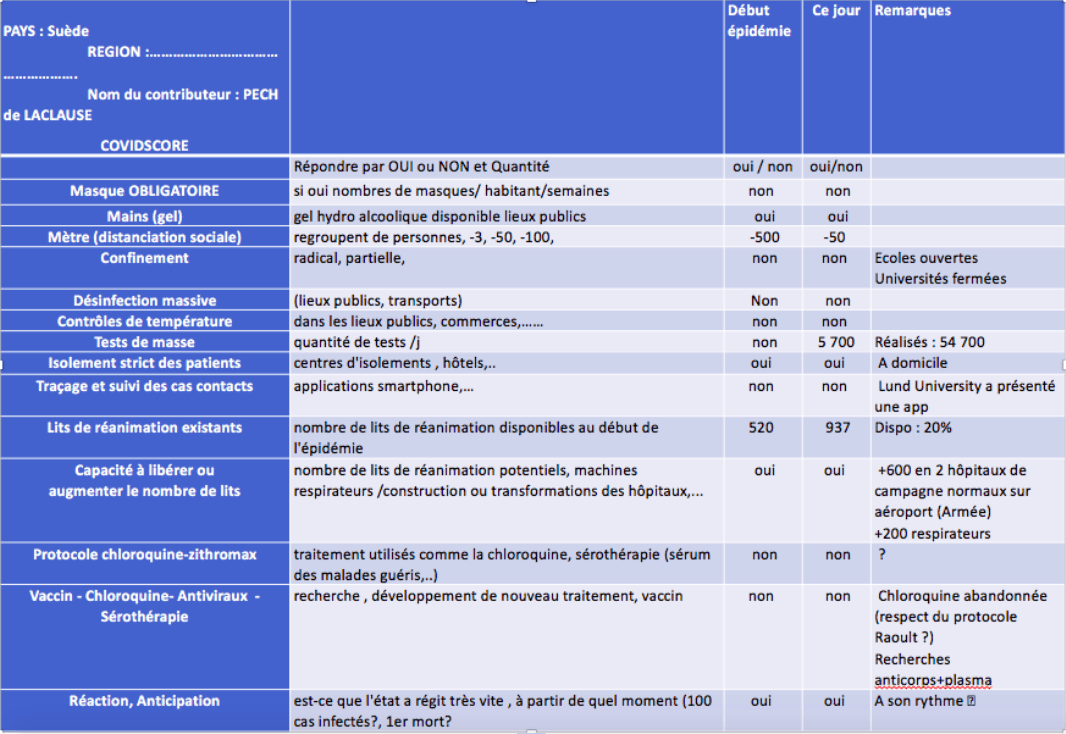
Nevertheless, there are four positive elements:
- The Swedes have protected the frail in an extremely effective way, which helps to explain the good résultats results in the future..
- Closure of some shops at risk(bars… universities, ski resorts and museums.
- Tests: policy in line with WHO recommendations.
- Construction of Covid medical structures, to deal with a potential overheating of the health system.
Note a Swedish specificity regarding the freedom left to citizens to assess their risk: physical distance, physique, travel, telework.
Ⅱ. A.3 Nevertheless take into account swedish specificity spécificité has three levels:
Low population density (contact): 2nd ème European country in terms of area (just after France) its population density is low (7 times less than France) with nevertheless 3″European”cities with important exchanges (cf Champion’s League): Stockholm, Gothenburg, Malmo
Large immigrant population: Sweden has always practiced humanitarian diplomacy with a large immigrant population (500,000 in Stockholm) in particular from Somalia
Culturally: very high level of human development (education) of this “Lutheran” population, known for three elements:
Strong individual responsibility: for example, low rates of regular consumption of antibiotics or anxiolytics compared to other European populations. Européennes.
Collective vision marked with respect for the other: few acts of incivility (metro fraud, pedestrian crossing respects, vandalism,..)
Intravert more than extrovert: far from our “Hugging or Kissing cultures” (Italy, France)
Ⅱ. A.4 Good results observed in Sweden: 2769 victims for 10 million individuals
At the global level, the results indicator currently available (evenmême if it has its imperfections in comby countriesas heterogeneous in terms of population density or practical tests or test declarations) tests) shows an excellent level of 27/100k individuals.
The distribution of mortality would be approximately: 40% in structures for the elderly,20% in the immigrant population (poor understanding of prevention messages initially in Swedish and English… ) and 30% in the general population (of course above all seniors).
The economic impact is estimated around -4% of the GDP.
Ⅱ. A.5 International and Scandinavian Comparisons(same ecosystem))
- At European level: As a reminder (see above I.6): the countries of southern Europe are moving to figures 10 times higher..
- At the Scandinavian level: the measurements of the other Scandinavian countries (green in the CovidScore) are still 6 times better (4-8/27)
Ⅱ. A.6 Can we conclude something:
We cannot conclude today of a better system than another, as the virus is still circulating, and that the Swedes have been more exposed to the virus (we will provide the rate of people immediately),and as a result theepidemic may last less in the long run.
Swedes get a good overall result, as:
- Fragile and vulnerable people have been protected effectively and preventively
- They believe that the collective immunity of their population is greater than that of their neighbours.
- The economy was less impacted than in other European countries.
II.B Europe: Countries that have decommated
II.C France – regional and departmental assessment: départementale :
II.C.1 Regional scissor régional effect:
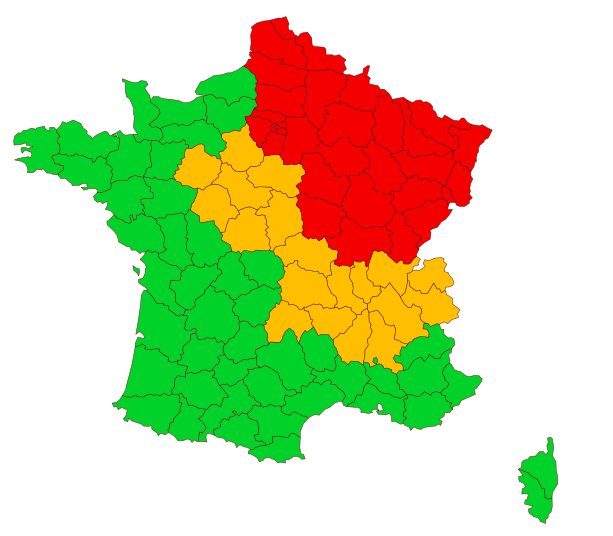
II.C.2 Preparing for deconfinement: East-West and North-South gradient
Ⅱ.D WORLD: Russia in epidemic phase and Africa surprises us
With the contribution of Dr. Bachir Athmani, Stéphane and Flavien Palero, companions of the first hour, whom I thank again for their unwavering support.
Beware of certain chiffres (number of cases, deaths…) extremely questionable because they vary from one country to another (example: availability of tests), with measurement biases and therefore a major under-reporting in some countries.
By continent
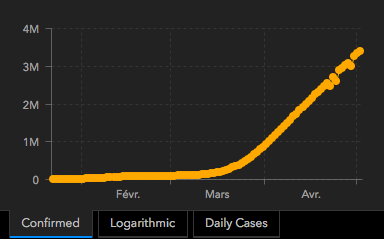
Ⅱ.D.1 Prevalence: 2.2 M of active cases confirmed for observation

Epidemic growth since January 1: Nearly 4 million cumulative cases
Geographical vison: 4 active poles: Americas, Europe, Middle East, Russia.
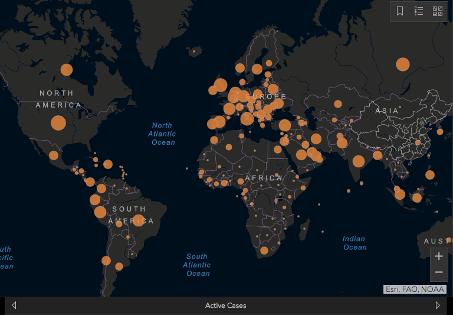
Note the very low number of deaths (example 15 deaths reported to date in Côte d’Ivoire) or cases of resuscitation in Africa (if resuscitation were full we would be): effect temperature/humidity, youth of populations, effect “quinine” … many questions still to be decided.
By continent: Americas, 50% of reported active cases, Europe 30%, Middle East and Russia has 7%

Top 10 countries
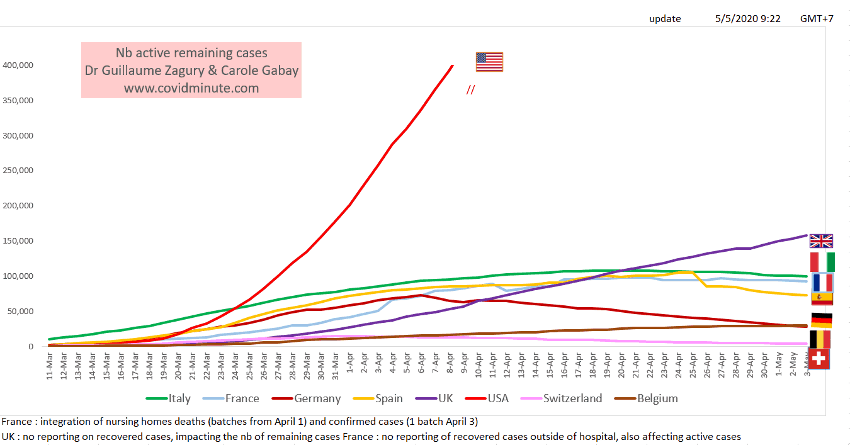
United States 958k (yesterday 939k)
United Kingdom 162k (yesterday 158k)
Russia 126k (yesterday 117k)
Italy 100k(yesterday 100k)
France 93k (yesterday 93k)
Spain 71k (yesterday 73k)
Turkey 56k (yesterday 60k)
Brazil 55k (yesterday 51k)
Netherlands 35k (yesterday 35k)
Peru 32k (yesterday 31k)
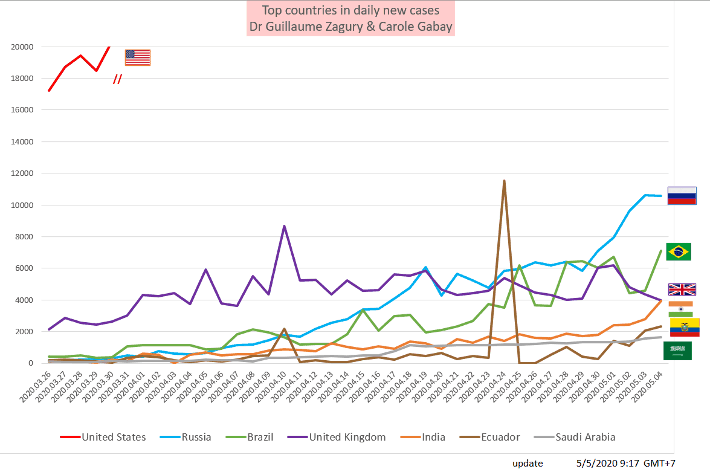
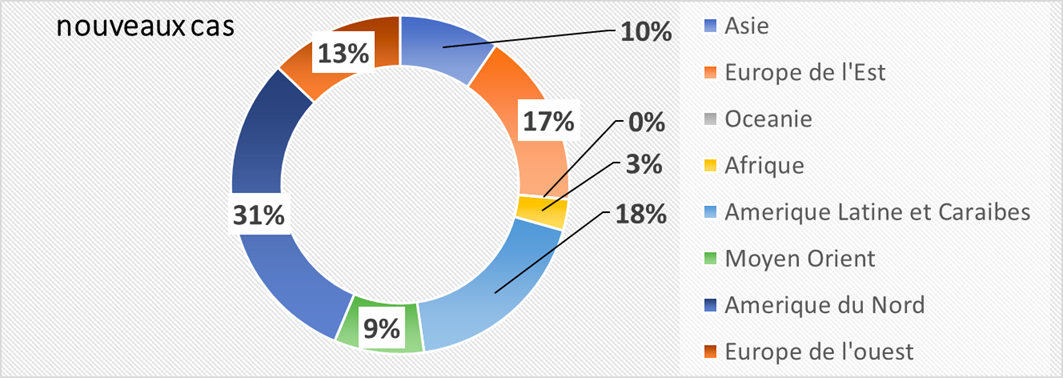
Ⅱ.D.2. Incidence: 76,000 new cases detected yesterday and Russia in epidemic phase(nearly 20% of new cases reported))

Depending on the weather:
Title: Impact of Reported Cases / World: Evolution Since the Beginning of theEpidemic
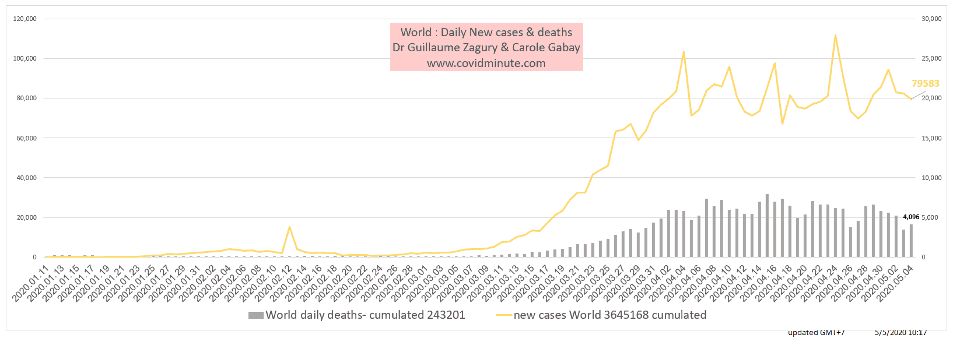
Geographical
Continent: more new cases in Russia than in Europe
By Country
United States 22k (25k yesterday)
Russia 11k (11k yesterday)
Brazil 7k (5k yesterday)
United Kingdom 4k (4k yesterday)
India 4k (3kyesterday)
Turkey 2k (2k yesterday)
Peru 1k (3kyesterday)
Canada 1k (3kyesterday)
Spain 1k (2k yesterday)
Pakistan, Singapore, Iran, Saudi Arabia, Qatar, United Arab Emirates, Bangladesh, Belarus, Ukraine, France, Italy, Ghana, Mexico, Chile, Ecuador: 1 to 2k
3 Countries Impact of Diagnostic Cases/MillionIndividuals:
Indicator very questionable because test dependent…
Keep in mind the “3M reflex” (Hands-Masques-Metre) to protect yourself… but above all to protect the most vulnerable.
Confidence and solidarity for this collective struggle
Dr Guillaume ZAGURY
- “Allsuccess is collective,”thanks to:
- The entire “Medical” team of “GCMN” type (Global Covid Medical Network): Dr. Bachir Athmani, Dr. Marc Abecassis, Dr. Mohamed Fadel, Dr. Jean Michel Serfaty, Dr Ibrahim Souare, Dr Jonathan Taieb…) that make this project a muste,
- The entire data analysis and IT team: Carole Gabay (“Data Analysis Expert”),Richard Coffre (exceptional webmaster), Flavien Palero (digital manager), Mathieu Bouquet (for his pastcontribution)
- The whole “Communication” team(Flavien Palero, Laetitia, Marie, Alison… ” ( ): without whom this project would not have been possible.
- All historical financial patrons (JeromeJérôme, Benjamin Denis and the Consulting CompanyB Square, Benoit Rossignol, Arnaud Bricout and TAG Advisory and Gilles Langourieux…) working for “Citizen Actions”
- We also thank the Paul Foundation
- If you feel like a patron or partner to finance computer development (all the others have been volunteering for 88 days!), please contact me (guillaume 888@hotmail.com).
- Also, our team, although partly based in Shanghai, will be delighted to welcome you … because it is not the work that is missing… !
[DISPLAY_ULTIMATE_SOCIAL_ICONS]
