Doctor Guillaume Zagury, live from China, shares his Chinese experience (SARS 2003 and 2 months of daily monitoring of the coronavirus epidemic in China), to try to better understand the situation as a whole.
The observations engage only itself and many other analyzes exist, which will help you to form your own opinion.
A. Strategy for France
Criticism after the fact, when historical elements are available, is easy. The goal here is not to blame anyone (because our health authorities are mostly made up of great people). It is rather a question of providing elements for the aftermath and raising awareness of the need for a rapid reaction, which is the key to success in the face of such an epidemic, as the various countries of Asia have shown us, each in their own way.
1. Failure to prepare
1.1. Shortage of basic equipment (masks, protective clothing, tests, etc.)
The shortfall is both quantitative, due to the weakness of strategic stocks. Other countries, including the United States, are in a similar situation, so it is necessary to put French improvisation into perspective and to question the process that led to this situation overall.
The insufficiency is also qualitative, insofar as France and most of the western countries have become dependent on Asia (for reasons of cost reduction, among others) in areas strategic for public health: biology (tests) and pharmacy (antipyretics, antibiotics, …), among others.
1.2. A just-in-time hospital sector
This situation is the consequence of the reduction in the number of beds for 20 years, in particular resuscitation beds, in a logic above all accounting.
1.3. Sometimes late and not always homogeneous decisions
Authorization of meetings with variable geometry (5,000 people, 30,000, …) and sometimes contradictory with authorization of assembly of different types:
- religious (as in Colmar),
- sports (PSG match behind closed doors but authorization to rally supporters outside the stadium, maintenance of the Lyon-Turin match while large rallies are prohibited and the epidemic is spreading in Italy, etc.)
- citizens (maintenance of the first round of municipal elections while confinement is outlined, demonstrations on the public highway, etc.), due to the taking into account of socio-political-economic data, considered more restrictive than the health threat.
It will be interesting to observe the evolution of the epidemic, and especially that of the use of resuscitation beds and deaths between Portugal (rapid and total measures) and Spain (or even France) where the reaction has seems to have been more progressive.
1.4. Three French specificities compared to countries that have mastered the epidemic (see our Covid-score table)

Let us first mention two key elements on which our country has, in my view, failed very specifically, but where it is possible to correct the situation:
1. Lack of precision in identifying cases: patients often go to their general practitioner, who cannot perform “minute tests” (or such tests have been developed in Vietnam or Thailand, countries which do not have the means of France!)
2. Return of patients with little or no symptoms at home: in practice, the general practitioner most often sends the patient home with the minimum advice (antipyretic, mask if available, follow-up)
However, this is an extremely risky approach, which inevitably generates family contamination despite all the precautions taken. The pathology is very contagious (as illustrated by the case of the liner Diamond Princess where despite the confinement in the cabins about 20% of the people on board were contaminated in less than 2 weeks).
All Asian strategies have focused on quickly identifying cases (tests available) and then isolating them in dedicated structures. The famous hospitals built in a few days in Wuhan were mainly intended to isolate positive patients from their family environment, until their contagiousness subsides.
It seems that Spain has started to mobilize hotel infrastructure to house Covid patients, with the aim of reducing intra-family contamination.
Last specific point on which France can do better:
3. Weak monitoring of contact persons: strict monitoring of all contact persons has proven to be extremely fruitful in Asian countries, even if it may sometimes appear to be liberticide at first (location via cell phone, imposed quarantine, etc.) . All contact persons should be placed under surveillance for 14 days (at home if negative, in dedicated structures such as requisitioned hotels if positive). The digressions on (temporary) liberticide measures should not prevent action. A democratic country like South Korea has used it successfully.
When there is a fire, we put it out first, then we debate!
2. The protective dike has failed and we are in an invasive phase
Containment has slowed viral spread, but it continues, especially among caregivers and within households.
Our healthcare system will have to struggle (5% of Covid patients will have to spend 2 to 3 weeks in intensive care) intensively, with the risk of exposure of healthcare staff (at least 6 healthcare providers already deceased) and exhaustion of human resources .
All of this teamwork is to be commended, as a hospital covers over a hundred distinct functions.
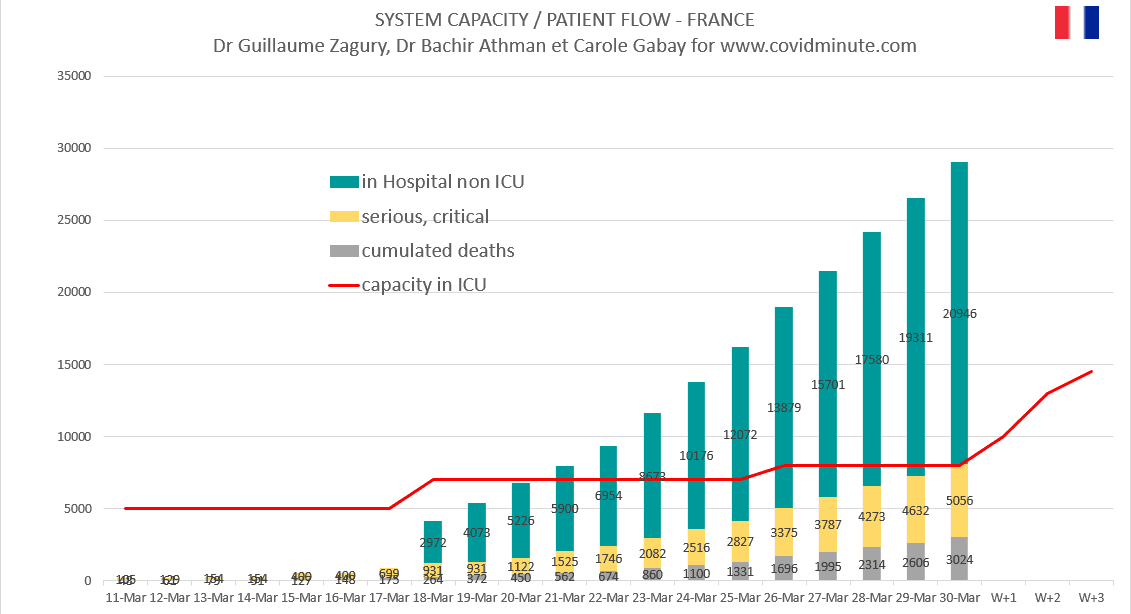
3. Short-term risk: saturation of the system
The following diagram clearly shows the challenges. We can quickly go from 7 to 14 or even 20,000 resuscitation beds, but the limit will be on human resources (in particular nurses) and certain equipment (difficulty in finding ventilators, even in China, due to global demand !).

4. Immediate strategy in the face of the inevitable medium overload of the system
4.1. Identification of patients at risk of death
80% of mortality in France is concentrated in those over 75 years of age.
99% of deaths in Italy present a high age or a comorbidity (respiratory, immunosuppression, morbid obesity,…).

4.2. Rebuild a waterproof protective dike for this target (the most vulnerable)
– prevention: strict confinement at home (the risk in case of contamination is to spend 3 weeks in intensive care) and establishment of isolation structures for positive patients, as a priority for nursing homes
– regular identification of cases (generalization of tests)
– protection of vulnerable people by equipping caregivers and contacts with ad hoc outfits
4.3. For the general “healthy” population
Containment with variable geometry and protective measures (for activities whose continuation is essential: transport, food, security, etc.) and telework. Different models have already been tested (in Hong Kong, South Korea, etc.) and allow us to see the results obtained. We will propose some standards to remember, with the update of our Covid-score table.
5. Containment release: not too early
The following are the recommendations of our team, based on what we have observed in Asia. These elements engage only us, and different strategies are obviously possible.
5.1.Resuscitation beds
Leaving confinement is not possible before seeing the occupancy rate of intensive care beds decrease (most deaths occur 3 weeks after the onset of symptoms). This rate is one of the few objective indicators of the health system’s ability to cope with the epidemic.
5.2. Protective equipment
The recovery of protective stocks, ideally for the whole population, is crucial. We expect a minimum consumption of 40 million units per week.
5.3. Measuring the epidemic
– Obtaining precise epidemiological data by region (requires better case detection)
– Serological tests to assess the possibility of collective immunity of the population
5.4. By step
Gradual reopening of activities.
In China, areas barely affected by the epidemic (Tibet and Qinghai provinces) resumed normal operation in early March. The moderately affected regions (almost all of the rest of China except Hubei) have gradually reopened public places then meeting places (restaurants, bars, etc.), schools are still closed, more than a month after the end of confinement!
5.5. Therapeutic progress
The results of the various therapeutic trials in progress may have an accelerating effect on the lifting of the containment, in the event that treatments show very favorable results.
NOTE: the epidemic is well covered by the French media on a daily basis. We now offer you our “minute diagrams” to make your own assessment of dynamic elements and trends, so as not to participate in over-information!
B. France D15 – Flow management
The elements below are to be read with the reservations concerning the validity of the data (case definition, possible underestimation, etc.) already mentioned above, and keeping in mind that it is the trends that count, rather than the raw figures taken at time t.
1. Incidence: 4,376 new confirmed cases (2,599 yesterday, 4,611 the day before)
We are still in the epidemic growth phase. The fall in the number of new cases on Sunday was not confirmed yesterday.
2. Prevalence: 33,599 active cases under observation (30.4k yesterday)
On this basis alone, the doubling time stands at 7 days, it seems to be gradually increasing over the past few days. This trend remains to be confirmed in the coming days.
3. Trend (comparison with Italy): close trajectory
The trajectory of France seems to be slowly moving away from that of Italy with a 10-day lag, but this trend remains to be confirmed by comparing the number of tests carried out by the two countries, data currently unavailable.

4. Territorial distribution: always Ile de France and Grand Est
A new counting method is being implemented, with an expected significant reassessment of the number of cases following the authorities’ declarations (announcement by the Ministry of Health on Saturday March 28). The figures by region will be provided in a more usable way for everyone in a few days.

C. World impact: an exponential dynamic
Thanks to Stéphane, a companion from the start, for his participation.
Of course with all the necessary reservations about the validity of the figures (availability of tests, validity of the data, etc.), but what is essential is the trend.
1. Incidence: 64k new cases diagnosed (59k yesterday, 67k the day before)

This is around 20 times the figures observed in China (around 1 / 5th of the world population) at the time of the peak in Hubei (3k per day, according to official figures).
2. Spatial vision: 80% of new cases remain detected in the West (50% in Europe and 30% in the Americas)
2.1. By country
The United States and Spain remain in an exponential phase.
- USA 20k (+2)
- Spain 8k (+1)
- Italy 4k (-1)
- France and Germany 4k
- Iran and England 3k
- Canada, Turkey, Switzerland, Netherlands, Belgium 1k
Table: evolution by country

Chart: evolution by country

2.2. By continent: ⅓ new cases in the Americas

D. Prevalence world
1. Figures (active cases): 580k (538k yesterday, 490k the day before)
The doubling time is 6 days (stable).
2. Spatial vision by country

Top 6 countries :
- United States 155k (135k yesterday), more than 25% of active cases on the planet
- Italy 76k (74k yesterday)
- Spain 63k (59k)
- Germany 53k (52k)
- France 34k (31k)
- Iran 25k (23k)
Thanks to Mathieu Bouquet, partner from the start, for his precious help.Virus Preventions 4 W’s:
Wear a mask, Wash your hands, Watch out for sick people, Wait for new updates from covidminute.com !
Protect yourselves, and above all protect the most vulnerable!
Dr. Guillaume ZAGURY,
Specialist in Public Health and Health Innovations
Consultant at “Health Innovations”
HEC
In China for 20 years“All success is collective”, thanks to:
– the whole “Back Up” team (Mathieu Bousquet, Carole Gabay, Flavien, Marie, Laetitia, Anne-Sophie, …), without whom this project would not have been possible.
– all the “Medical” team (Dr Bachir Athmani, Dr Ibrahim Souare, Dr Taieb, Dr Viateur …) who allow this project to exist,
– all historical financial sponsors (Jerome, Benjamin Denis & B Square, Benoit Rossignol, Arnault Bricout) who work for “Citizen Actions”
If you feel like a patron or of partners to finance IT development, don’t hesitate to contact me (guillaume@covidminute.com).
Also, even if part of the team is based in Shanghai, do not hesitate to come and join us, because there is no shortage of work :-)If you want to find more analyses and infographics, follow our account at:Know the latest updates
Powered byMedicilline