We know that many journalists and decision-makers (“crisis cells”, ministries, etc.) read this analysis “served at breakfast”, and we are delighted. We just ask you, when you use our ideas or illustrations, to have the courtesy to quote us.
Doctor Guillaume Zagury, based in Shanghai, specialist in international public health and in health innovations, comments for the Community day by day the evolution of the epidemic for more than three months, and delivers in preview the elements of understanding on its “country & region analysis” and foreseeable consequences (experiences of SARS in 2003 and of Covid-19 in China).
A whole remarkable multidisciplinary volunteer team allows the realization of this analysis which wants to be factual and objective (moreover, do not hesitate to join us: mail below): “all success is collective”.
Beyond the voluntary skills, this project was made possible by the support of our patrons with a civic vision: the Paul Bennetot Foundation (Matmut Foundation under the aegis of the Fondation de l’Avenir), B Square, Tag Advisory , Daxue Consulting, as well as various fellow travelers (Jérôme, Dr Benoît Rossignol, Gilles Langourieux, …)
Our illustrations, created almost 100 days ago, will soon be available on our site and you can download a large part of them. (www.covidminute.com).

I. COVID “360 ° MINUTE”: 2 maps and 4 graphs (=> 80% of useful information)

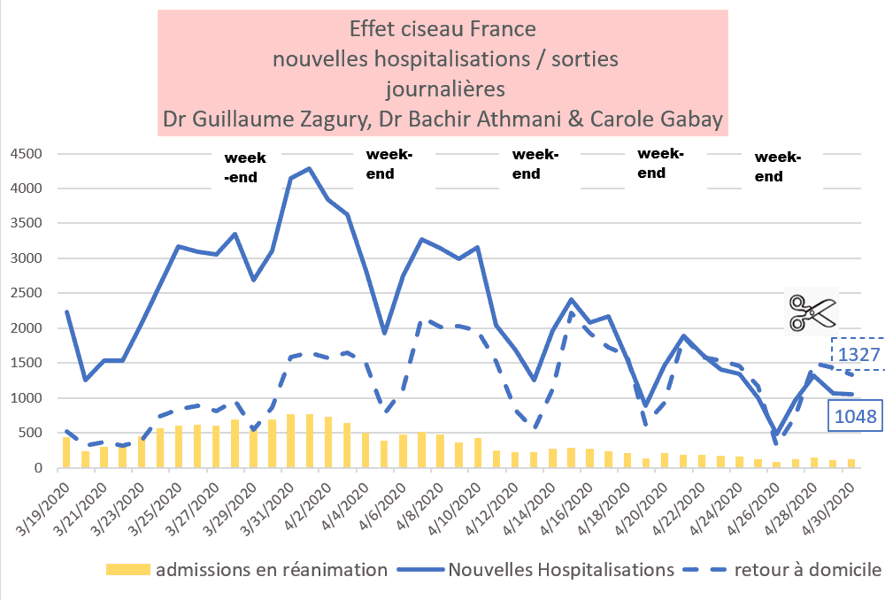
1. France – a favorable but slow dynamic
Scissor effect in progress (hospitalizations & resuscitation) with nevertheless still 1000 hospitalizations / day (after more than 40 days of confinement)
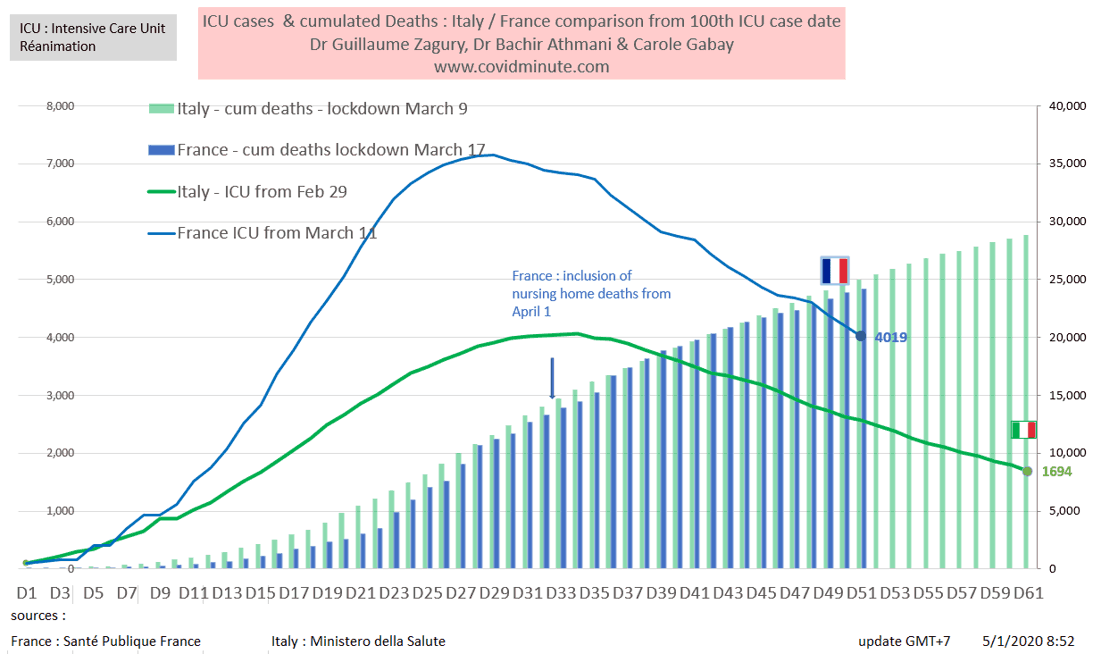
2. Time vision: we are following Italy 10 days later
Comparative chronological evolution of resuscitation cases France / Italy
3. France – Provisional: resuscitation beds available (the stake from May 16)
Post-deconfinement projection, based on 3 elements: historical data, incubation time (D7 with an expected increase around May 16), and the influx of patients C (-)


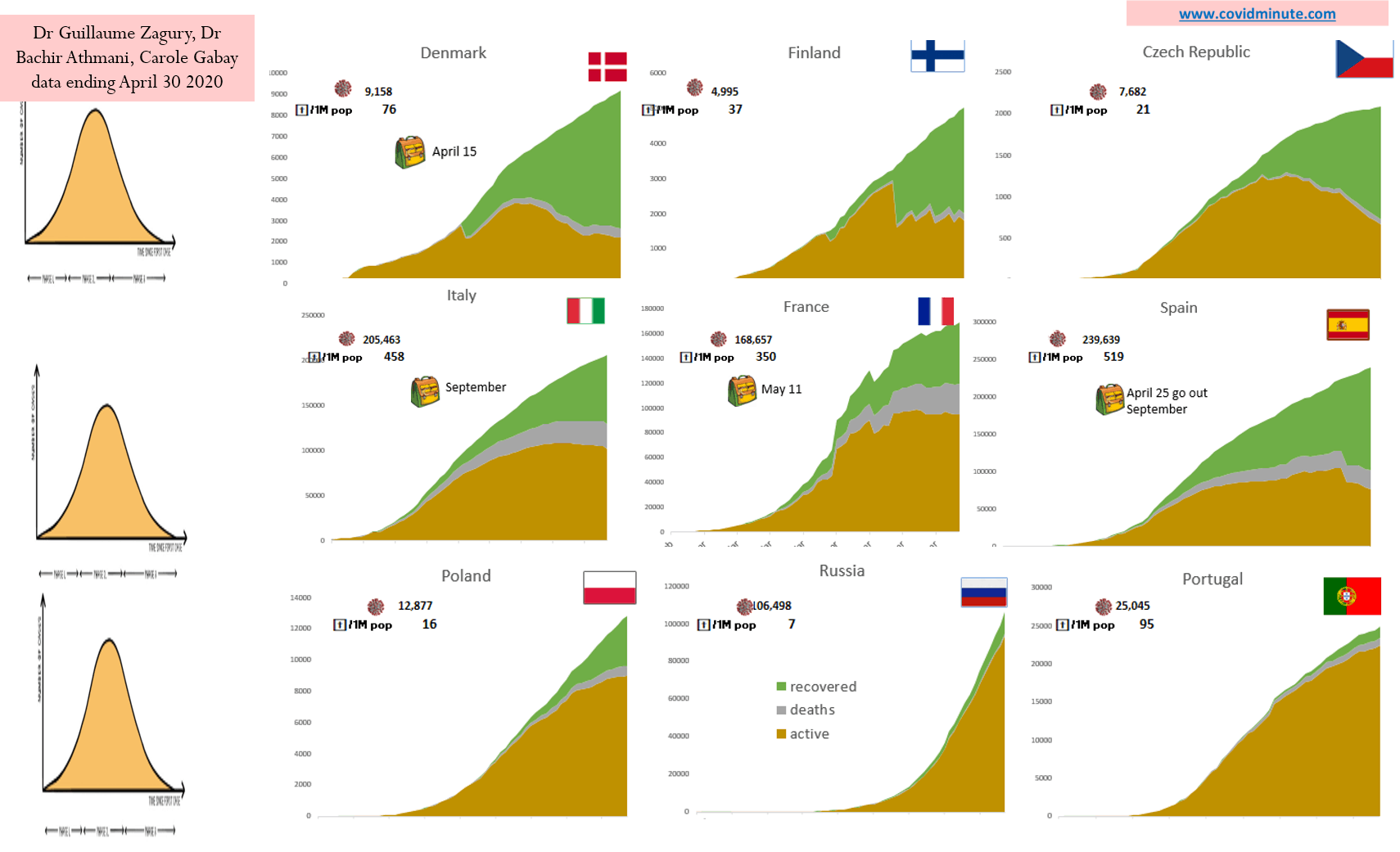
4. 3-speed Europe: peak – plateau – epidemic phase
Community countries in epidemic control phase:

5. Globally
Half of the 2 million active cases in the Americas and a third in Europe: monitor Russia and Brazil


A.Good morning Asia: Possible 2nd wave in Singapore mainly among migrants (⅘ of active cases)
I thank my friend Arnaud Favry at Singapour, member of our international network, for sharing this information with us.
A.1 Singapore Digest: to understand
Population: 5.5 million
About 330 K migrants (6% population) often English-speaking (Nepal, Sri Lanka,…)
“Ming Gong” type migrants in China: with very difficult accommodation conditions (12 per dormitory) ….
Despite its geographic and economic proximity to Mainland China the first case is only detected at the end of February.
A.2 Good initial management with a “Kit Test” Country
The 1st wave was well managed with a proactive attitude: Test-Tracing-Temporary exclusion
To date, 21,000 tests / million inhabitants have been carried out.

A.3 But a second wave appeared at the end of March, with currently 15,000 cases (including 12,000 migrant workers and 3,000 natives), for three reasons:
- Late closing of borders to already endemic countries (USA, England, …):
- While the country had closed its access to European Companies, it only closed them later for American and English companies.
- This without any screening measures on arrivals
– Now we know that +/- 50% of patients are asymptomatic.
-Migrant workers with little or no testing
– Late resort to wearing a mask: compulsory only at the beginning of April
Recall that the City has a dual culture historically speaking: Anglo-Saxon (no mask) and Chinese (mask) essentially.
As much as the WHO recommended it without further ado
A.4 Rapid reaction of the authorities: along 4 axes
- Containment of the population
- Mature quarantine of 300K migrants under army control
- Mass tests in particular on the migrant population (¾ of the cases) at high risk of contagiousness (promiscuity, …): the capacity in tests thus went from 3k / day at the beginning of April, to 8k / day currently.
- For positive cases: provision of isolation structures (18,000 beds) and hospital beds (23,000) within less than 2 months.
A.5 A cultural exception which is coming to an end: the wearing of the compulsory mask came into force on April 15.
In early April, the Prime Minister offered all citizens a reusable mask to collect at a community center.
A.6 Results indicators:
For the Aboriginal population: change to less than 20 new cases / day and the objective is less than 10 / day the week of May 4, and in this case lightening of the current confinement.
Mortality (15 deaths to date): one of the key indicators is the number of deaths / Million inhabitants and amounts to 2.6 / Million inhabitants (France 353 / M). It should remain low, because the populations currently reached are young (migrant workers)
Resuscitation: the capacities in intensive care beds (+/- 1200 beds) have never been saturated.
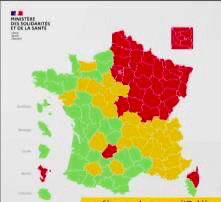
B. France: The epidemiological map of deconfinement:
2 indicators and a synthetic map with its East / West and North-South gradient
B.1 Viral circulation: only 5 departments with negative dynamics

B.2 Resuscitation capacities to absorb a second shock: occupation of resuscitation beds

B.3 In total: An East-West and North-South gradient to be monitored regularly

C. WORLD: 4 billion confined, 3 million historical cases declared, 2 million active cases (and soon 200 k deaths)
With the contribution of Dr Bachir Athmani, Stéphane and Alison, companions from the start, whom I thank again for their unfailing support.
Beware of certain figures (number of cases, deaths, etc.) which are extremely questionable as they vary from one country to another (example: availability of tests), with measurement bias and therefore major under-reporting in certain countries. .
C.1 Prevalence: United Kingdom 2nd country in terms of prevalence
Chronological evolution: 2 million active cases declared and 3 million historical cases
2,031,000 active cases confirmed under observation

Epidemic growth: 3 million historical cases

Space vision: 4 active hubs: Americas, Europe, Middle East, Russia.

By continent: Americas, 50% of active cases declared, Europe 30%, Middle East and Russia at 7%

Top 10 countries: United Kingdom 1st European household
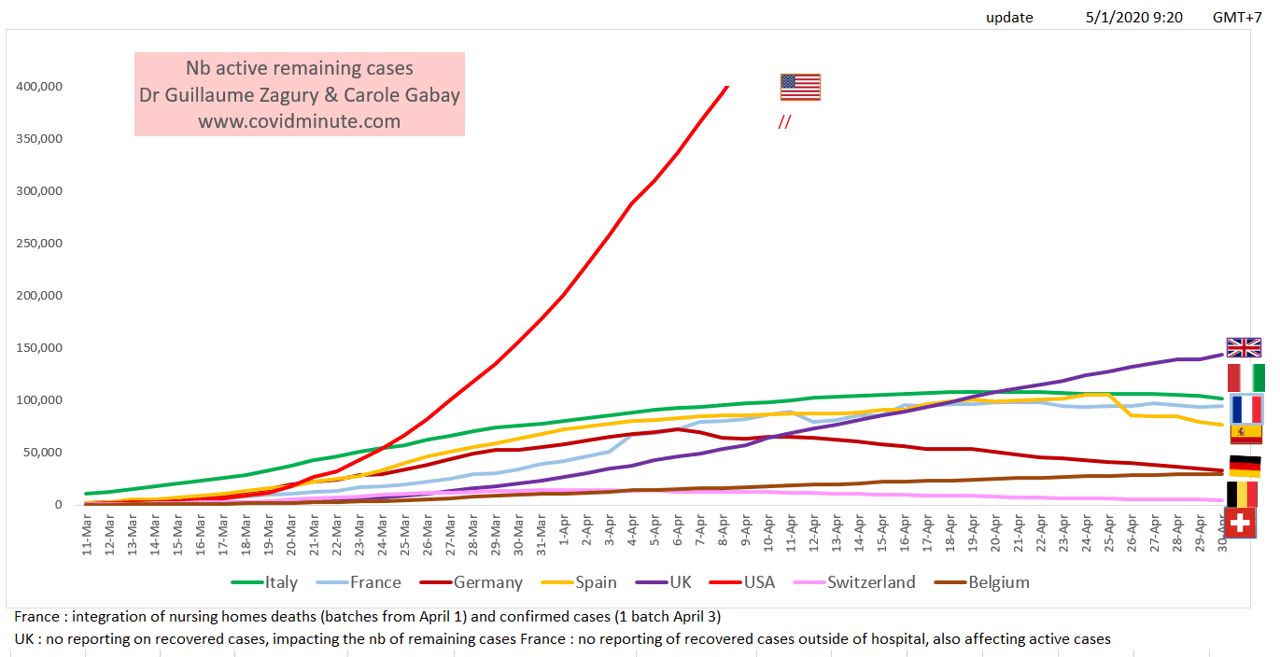
Top 10 countries
United States 879k (yesterday 850k)
United Kingdom 144k (yesterday 139k)
Italy 102k (yesterday 105k)
Russia 94k (yesterday 88k)
France 93k (yesterday 94k)
Spain 77k (yesterday 80k)
Turkey 68k (yesterday 70k)
Brazil 44k (yesterday 39k)
Germany 33k (yesterday 34k)
Netherlands 34k (yesterday 34k)
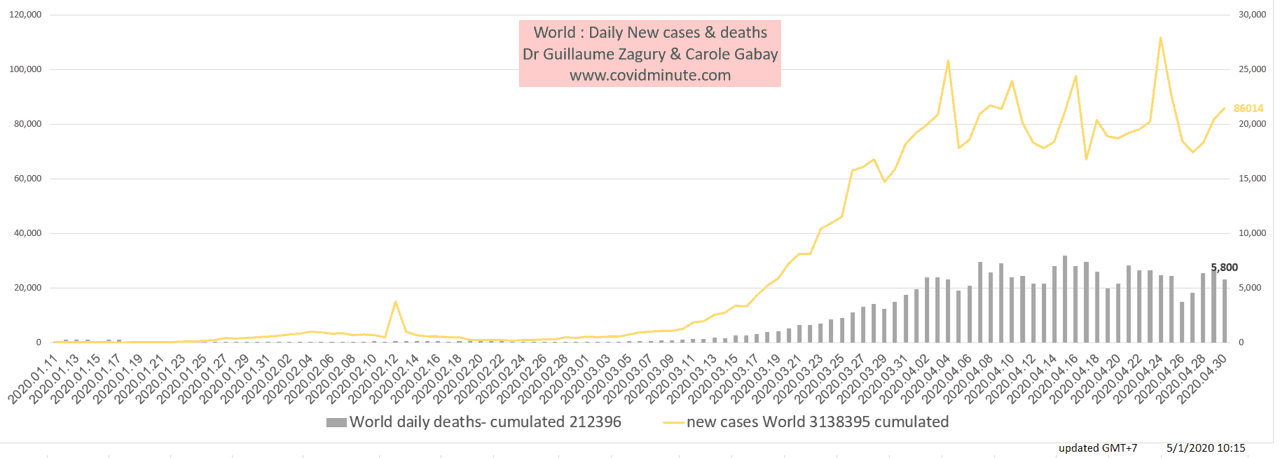
C.2 Incidence: viral recovery
Chronological vision:
Incidence: 85,000 new cases detected yesterday
By continent: Brazil and Russia are in the epidemic growth phase and are joining the United States.
Top 10 countries: new active households in addition to the USA: Russia, Brazil, United Kingdom, …..
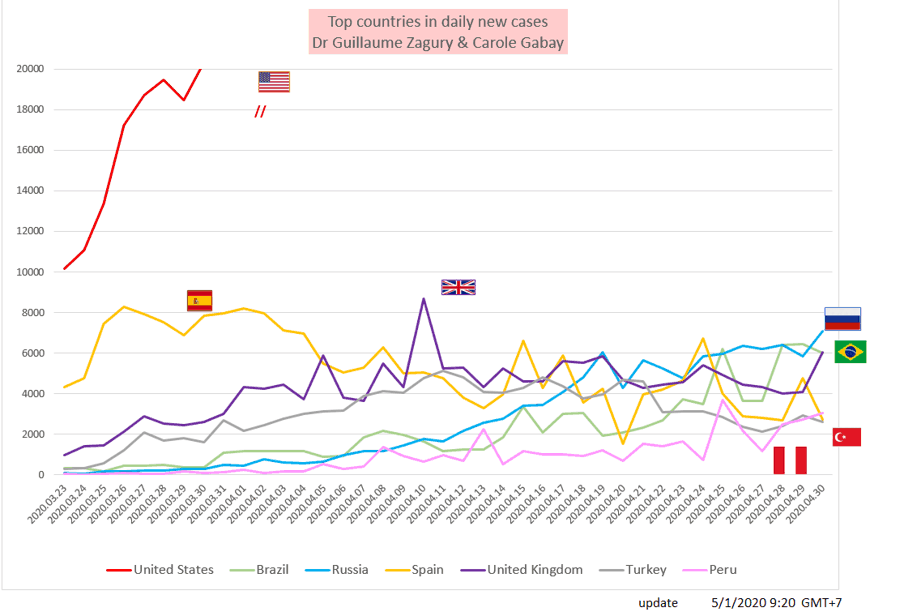
United States 30k (21k yesterday)
Russia 7k (6k yesterday)
Brazil 6k (5k yesterday)
United Kingdom 6k (4k yesterday)
Spain 3k (5k yesterday)
Turkey 3k (3k yesterday)
Peru 3k (3k yesterday)
India, Singapore, Pakistan, Iran, Saudi Arabia, Qatar, United Arab Emirates, Bangladesh, Belarus, Ukraine, France, Belgium, Germany, Sweden, Italy, Portugal, Canada, Mexico, Chile: 1 to 2k
C.3 Let’s monitor one of the outcome indicators: the number of deaths per million inhabitants
“Gross” table: behind the figures…. variable geometry strategies

The West gathers 90% of the declared World mortality (200k deaths, including more than 100k in Europe and more than 60k in the United States), and more than 90% of the declared cases (see dependent tests). in Hubei was underestimated in the initial period, and comparisons will obviously be difficult.
Keep in mind the “3M reflex” (Hands-Masks-Meter) to protect yourself… but above all to protect the most vulnerable.
Trust and solidarity for this collective fight
Dr Guillaume ZAGURY
“All success is collective”, thanks to:
the whole “Medical” team of the “GCRMN” type (Global Covid Medical Network): Dr Bachir Athmani, Dr Marc Abecassis, Dr Marc Genton, Dr Mohamed Fadel, Dr Emily Kara, Dr Ibrahim Souare, Dr Jonathan Taieb, ,,. ..) that allow this project to exist,
the entire data analysis and IT team: Carole Gabay (“Data Analysis Expert”), Richard Coffre (exceptional webmaster), Flavien Palero (digital manager), Mathieu Bouquet (for his past contribution)
the entire “Communication” team (Flavien Palero, Laetitia, Marie, Alison, …): without whom this project would not have been possible.
all financial sponsors including the Paul Bennetot Foundation (foundation of the Matmut under the aegis of the Fondation de l’Avenir), Jerome, Benjamin Denis & Société de Consulting B Square, Benoit Rossignol, Arnaud Bricout & TAG Advisory and Gilles Langourieux who work for “Citizen Actions”
If you feel like a patron or of partners to finance IT development (all the others have been volunteers for 88 days!), Don’t hesitate to contact me (guillaumez888@hotmail.com).
Also, our team even if partly based in Shanghai, will be delighted to welcome you … because there is no shortage of work …!
[DISPLAY_ULTIMATE_SOCIAL_ICONS]
