Doctor Guillaume Zagury, based in Shanghai and specialist in international public health & “health innovations”, comments with his volunteer and multidisciplinary team, the evolution of the epidemic for 68 days…., And gives us a sneak preview understanding of the foreseeable consequences.
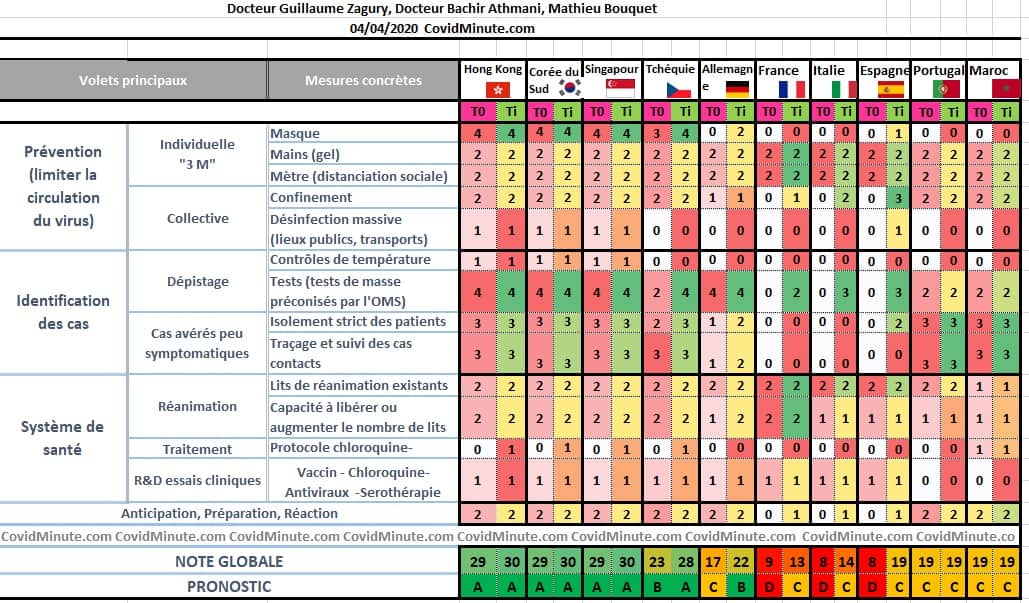
A. SYSTEM APPROACH = “COVID MINUTE” TABLE: West, 360 * turn on masks (= mobile confinement)!
1. The American CDC and the Academy of Medicine in France strongly recommend wearing the mask.
– Change of course, since the infection is recognized essentially by “airborne transmission” … and thus the mask becomes from: “little recommended” to almost mandatory.
– I presented you on a video yesterday, daily life in Shanghai during an epidemic, and we can see that it is well accepted by the population and effective
– It is one of the flagship measures of Asian success (also a Central European country like the Czech Republic)
2. The mask: not to protect yourself, … but to protect others!
3. We are too dependent on Asia and China!
China, good at its gradual economic recovery, has transformed its industrial apparatus into a factory on the planet (one of the advantages of the system is its reactivity!).
Note that China makes it an asset:
– diplomatic (“Soft Power): since neither the USA nor Europe can provide concrete elements to Africa
– commercial: with sales and a unit price sometimes multiplied by 25, compared to previously (Great opportunity lost by China to show that its relations were not only “Business oriented”!).
4. Even light protection is better than nothing at all!
– different types of mask depending on the risk of exposure. For example, in Asia: N95 equivalent to our FFP2 for resuscitation doctors, K95 for nurses, and surgical for the general public ..,
– There are a multitude of tutorials on the Internet
5. COROSCORE leading countries all adopted this measure very early
– Asians: for reasons already seen: cultural (pollution or aesthetic) and historical (Sars 2003)
– European countries: in particular the Czech Republic (measure imposed since March 15), Slovenia, Austria, …
– Some countries, like Israel, which practice it for those who come out of confinement.
6. The Czech case: system approach (see iconography) explaining the current global score at 28/30.
– The Czechs play on all fronts simultaneously with a proactive attitude and not by adapting to the epidemic.
– Thus: masks (18/3), massive diagnostic kits (23/3), tracing on smartphone (30/3), release of energy on potential therapeutics and of course supervised (serotherapy authorized on 30/3)

B. Digital tools for mobile “confinement”:
1. Numerous digital applications and tools based on geolocation, Artificial Intelligence, even virtual reality, will help diagnosis and especially secondary prevention: referral of patients according to symptoms, follow-up of Covid plus cases, etc…
2. They have proven themselves in many Asian countries, such as “KakaoTalk” in South Korea, with real-time visualization of Covid plus patients, …
Some countries even go very far (see too much!), With the installation of an electronic tool on the doors of patients in their fortnight in Shanghai (see our analysis from 10 days ago)
3. In France, we can quote applications of this type, which are currently being developed (Track Vir, etc.)
4. The urgency is with the development of this type of tools and their use: this will make it possible to lift the massive and non-targeted containment measures (XXth century)
=> with mask, tests and immune status,
=> the economic impact could probably be thus limited
C. France D19 – Still in epidemic phase
Analysis with the contribution of Dr Bachir Athmani.
The elements below are to be read with the reservations concerning the validity of the data (case definition, possible underestimation, etc.) already mentioned above, and keeping in mind that it is the trends that count, rather than the raw figures taken at time t.
1. FRANCE : the 6 numbers to understand:
6,662 cases in intensive care (+ 641 yesterday) with a capacity of 14,000 beds; it is the all-time record for France.
64.3 k confirmed cases cumulated by PCR tests (+ 2.2k in 24 hours).
27,432 hospitalized cases (+ 1.2k cases in 24 hours).
914 resource health establishments, compared to 880 yesterday. Private establishments are finally called upon to contribute to the common effort.
6,500 deaths
2. Evolutionary dynamics: quite comparable to Italy
– However, be careful, there are a lot of insufficient elements in the count: you have to compare what is comparable, which is difficult in the current state of available information. Among other possible elements of measurement bias: death outside hospitals (among others in nursing homes), Covid case of decompensation catalyst or case by pathological mechanism, etc.

3. Health system: hospital vision “resuscitation”
3.1. Hospitalizations
3,195 emergency visits yesterday for suspected Covid-19 (3,745 the day before)
40% were hospitalized and 4% were admitted directly to intensive care (these 2 percentages remain stable)
43.6 k tests (36k the day before) in the laboratory, including 30% positive tests. The tests are starting to be available, congratulations to the different contributing energies, because they are one of the keys to an effective strategy.
3.2 Resuscitation: the real current and future challenge of our system
6,017 cases are in intensive care (+ 452 cases in 24 hours).
Age (++): one of the admission criteria considering of course, physiological age and not purely chronological age:
- 1% (93 people) are under 30
- 4% between 30 and 60 years old
- 35% are under 60,
- 60% are between 60 and 80 years old.
The median age of resuscitation patients is now 58 years (decrease in age because we will not be able to accept all cases in resuscitation, in case the prognostic scoring – Apache type or other – will not be favorable) .
Our health authorities are accelerating the effort at the national level: more than 9,000 beds (or soon 14k) in intensive care are available today against 5,000 at the start of the crisis.
I offer you the explicit and visual graph (we had a computer bug yesterday!) On the state: load / capacity in France

A downside, because it is necessary to reason locally and in terms of load / capacity: we have 2 epicenters already at a maximum level of saturation: Ile de France and Grand Est. The following table provides a good understanding of the situation in terms of future regional “load / capacity” (it will be necessary to isolate the resuscitation beds / region to be precise):

– Hence our suggestion for 3 days: it would be preferable to limit transfers to the West from the IDF or the Grand Est, because they exhaust the teams (4-5 people for a patient), and create FROM NOW in Paris a AMS resuscitation of 1000 beds. You have to think ahead, because in a week it will probably no longer be possible to transfer patients to other regions.
This AMS of 1,000 resuscitation units can be single or two-headed (2 x 500 beds): Hôtel Dieu, Val de Grâce,…
3.3. Deaths :
– 5,091 people died in hospitals (+ 588 people) and 6,507 died counting deaths in nursing homes.
– 83% of the deceased are over 70 years old.
3.4. To be continued :
Three types of places are at major risk of epidemic spread:
1. Ehpad: 17,827 confirmed or possible cases. 66% of Ehpad have already reported an episode concerning one or more cases of Covid-19. The number of confirmed cases in nursing homes and medico-social establishments is at least 17,827 (1,416 deaths). As the episode of Mougins shows, extreme vigilance is necessary to protect these populations.
I will ask Carole to monitor these 2 key parameters on this extremely fragile and suffering population (both physical and moral (isolation!)).
2. Prisons: cases exist and affect both prisoners (promiscuity: 70k prisoners for 60k places) and supervisors.
3. Places of religious gathering (see examples from South Korea, Malaysia, Iran, Israel, Colmar): these places must remain closed for the benefit of all.
– Note the Israeli case: 50% of the Covid cases, concentrated on 10% of the population (“Orthodox” Jews with many children and living in close proximity), God being stronger than the virus; . Besides, the Minister of Health (!!) himself, “Ultra Orthodox”, is himself Covid +. We will see how the Start Up Nation will undoubtedly generate a number of technological innovations on the Covid.
4. Regional vision
Always the East-West gradient with an epicenter, the Ile de France.

D. World & “Geopathology” (term I created 2 months ago, to show the multidimensional implications of this pathology).
With the contribution of Stéphane, companion from the start.
The reported cases are unreliable data as they are very dependent on the layout of the tests, but other things being equal, the trend is an important element in decision-making.
As you are in “over-information” mode, some elements of understanding:
1. In brief (/ over information ..)
– 🌎 The West (Europe and the USA) accounts for 83% of existing cases, new cases and deaths.
– (US) The United States is the first country affected in terms of diagnosed cases (29%): 257k cases (including 40k cases yesterday) and 6.5k deaths (remember that deaths are generally postponed to S2-S3).
– (US) The US economy posted a record unemployment rate of 4.4% in March with more than 700,000 jobs destroyed. These precarious situations will accelerate the epidemic because access to care is one of the components of the “global” strategy (see table: COVIDSCORE).
– (IT) First signs of slowdown in Italy and Spain: the number of daily deaths has started to decrease in the last few days and there would start to be fewer new daily diagnostic cases (Italy). Let us remain cautious and await confirmation of this positive trend for all.
– (CN) In China, after 2 and a half months of strict confinement, the inhabitants of Wuhan will finally be “released” in 4 days and will be able to leave Hubei and join their families. As a security measure, they are not yet allowed to travel to Beijing, where precautionary measures remain maximum, even oppposite the other Chinese provinces (with the exception of some border areas of the capital).
2. Incidence : 81k new cases (10% of existing cases)
2.1. INCIDENCE : 81,000 New Cases (80k yesterday, 77k the day before yesterday)

Chronological vision:

Geographic vision:
By country (“Top 10”): America in exponential mode

USA 31k (+ 6k)
Spain 7k (-1k)
Germany 6k (-1k)
France, Italy 5k
England 4k (+ 0k)
Iran, Turkey 3k
Russia, Brazil, Portugal, Canada, Netherlands, Belgium: 1k
By continent: 83% of new cases are in the West

Analytics: Italy on a plateau? To be continued.

It seems that the slowdown is confirmed in Italy, which has been on a “plateau” for a few days.
3. Prevalence : 0,81 Million cases diagnosed under observation

– Doubling time around 7 days (stable)
Geographic vision: 82% of active cases in the West
Top 10 countries: including ⅓ in the United States which are gradually becoming the epicenter of the epidemic.
USA 256k
Italy 85k
Spain 77k
Germany 65k
France 44k
Iran and England 33k
Note: be aware that these figures are questionable barometers because of diagnostic tests, and so the figures for Africa (+/- 1.5 billion individuals) are probably well underestimated (measurement bias).

Vision “mapping” (John Hopkins Public Health School in Baltimore): 10 Wuhan in Europe or the United States.

By continent: with a doubling time around 3-4 days, America should be the epicenter next week.

4. Mortality
By country: we have prepared with Carole Gabay, our Data Analytic Manager, a table

More visually:

Note that the tip of France is linked to the inclusion of 884 deaths in nursing homes recorded since the beginning and presented yesterday.
E. TOMORROW: Technological monitoring
1. Now that our country is adopting a “system approach” (see Table A), I think that the delay will quickly fill up on “mechanical” type measures (masks, tests, etc.), and that the emphasis will be put on the tools.
2. As a specialist in Health Innovations, I will try to provide you with Anne and Bachir, the best “Covid” innovations that we could make available to professionals and to the population, both in terms of:
– biopharmaceutical, with different ongoing protocols: chloroquine-azithromycin, serotherapy (encouraging results in the USA), antivirals, and ultimately vaccine (Professor Gallo’s GVN project in Baltimore, …).
– practical: with many digital tools (besides our application is in progress and we hope you will find it useful in a few days!) including those listed above.
– It is shared technology and global knowledge, which will allow us not to have a “Spanish Flu” type assessment of 100 years ago (approximately 150M deaths in 1918-1919 for a population of 2.5 Billions of individuals)Virus Preventions 4 W’s:
Wear a mask, Wash your hands, Watch out for sick people, Wait for new updates from covidminute.com !
Protect yourselves, and above all protect the most vulnerable!
Dr. Guillaume ZAGURY,
Specialist in Public Health and Health Innovations
Consultant at “Health Innovations”
HEC
In China for 20 years“All success is collective”, thanks to:
– the whole “Back Up” team (Mathieu Bousquet, Carole Gabay, Flavien, Marie, Laetitia, Anne-Sophie, …), without whom this project would not have been possible.
– all the “Medical” team (Dr Bachir Athmani, Dr Ibrahim Souare, Dr Taieb, Dr Viateur …) who allow this project to exist,
– all historical financial sponsors (Jerome, Benjamin Denis & B Square, Benoit Rossignol, Arnault Bricout) who work for “Citizen Actions”
If you feel like a patron or of partners to finance IT development, don’t hesitate to contact me (guillaume@covidminute.com).
Also, even if part of the team is based in Shanghai, do not hesitate to come and join us, because there is no shortage of work :-)If you want to find more analyses and infographics, follow our account at:Know the latest updates
Powered byMedicilline