A. A strategic visual table: what for?
1. In no way to blame
In February, no one thought that such a tsunami would hit Europe.
Many specialists (virologists, epidemiologists, etc.) had issued a storm warning and not a tsunami warning.
As a result, the authorities anticipated on the basis of a storm and stocks were not up to par.
It would be easy to “redo the match” with the current data, but we will remain in our role of proposing concrete solutions.
The controversy is not in the middle of a viral war and we must remain grouped around our health and political leaders.
Moreover at this stage, it seems that the state of mind is changing and that the principles of precaution acceptable in peacetime (clinical trial, purchase of equipment with administrative brake, authorization to carry out biological tests , factory transformation to be less dependent on Asia,…) are now much more flexible and action-oriented.
2. To better understand the purpose: a table listing the best solutions identified (WHO, Asian countries, etc.)
They are preventive:
– “3M”, protective equipment for professionals, containment, etc.
– Identification and management of cases: tests, digital applications for tracing,…
They are curative:
– Human resources (nurses and resuscitation-type doctors)
– Number of resuscitation beds with ventilators,…
3. The updated table is divided into 2 parts T0 and Tn
It allows you to visualize the evolution of country strategies according to their specific means over time.

4. For transparency reasons, we have only kept countries whose data cannot be questioned at present
Hong Kong, Singapore, South Korea,…
5. Our rating system is based on reference figures (“standard” like “best practice”) which we will offer very quickly.
We have noted on the basis of elements published and currently brought to our attention in the different countries. Weighting is the result of our experience and can of course be discussed, but at least the reasoning remains the same.
B. France: within a week, saturation of the IDF and probably more than 10,000 cumulative deaths

1. Doubling of deaths every 4-5 days
Tendency to confirm, pending the upturn of all figures from Ehpad.
2. Next week may be difficult and we should reach 10,000 deaths around Friday
As a reminder, the assessment of the heat wave in 2003 was estimated at 15,000 deaths.
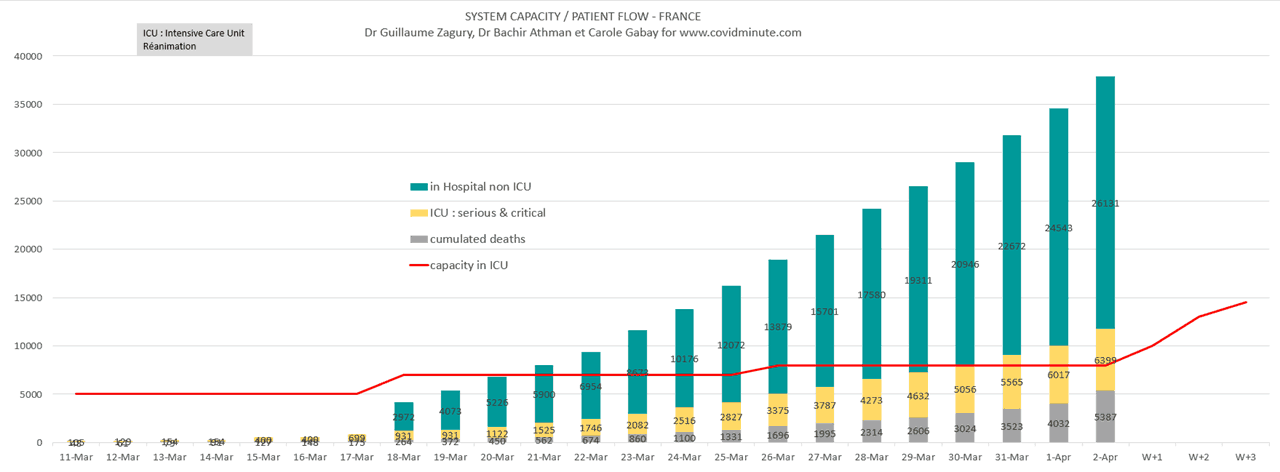
3. Resuscitation load / capacity
Quantitatively: exponential evolution of resuscitation cases.
Qualitatively: difficult care in certain regions (load / capacity): IDF, Grand Est
Resuscitation services could be saturated because there are still few outings to compensate for the daily influx.
Hence our proposal yesterday for the IDF with a PMA of 1,000 Covid resuscitation beds as a goal (at the Hôtel Dieu, in Val de Grâce,…), so as not to be surprised and to be proactive.
C. France D18 – Still in epidemic phase
Analysis with the contribution of Dr Bachir Athmani and Jonathan Taieb.
The elements below are to be read with the reservations concerning the validity of the data (case definition, possible underestimation, etc.) already mentioned above, and keeping in mind that it is the trends that count, rather than the raw figures taken at time t.
1. Numbers
6,000 cases in intensive care for a capacity of 14,000 beds, but we must reason locally and not nationally: the Ile de France and Grand Est regions are saturated, while other areas have not yet undergone the wave.
59.1k confirmed cases cumulated by PCR tests (+ 2.2k in 24 hours).
26,246 hospitalized cases (+ 1.5k cases in 24 hours).
880 resource health establishments, against 717 yesterday. Private establishments are finally called upon to contribute to the common effort.
12.4k recovered people have been discharged from hospital since March 1.
4,503 people died in hospitals (+ 471 people), a number to which must be added the 884 deaths probably linked to covid-19 in nursing homes (provisional figure).
A warehouse in Rungis market will be requisitioned to serve as a morgue.
An exit certificate will be available on smartphone next Monday.
Respect for hand washing, respect for confinement and barrier gestures, distancing, are the most important rules to respect.
2. Evolutionary dynamics compared to Italy
Number of cases (knowing that these data are highly questionable and depending on the number of tests available).

The absorption curve for resuscitation cases is more relevant. This type of graph will make it possible to observe the evolution of the various public health measures on the basis of more objective figures (not dependent on screening strategies).
– Apparent stabilization of resuscitation cases in Italy (especially in Lombardy and Veneto where the first confinement took place, but it is advisable to remain cautious.
– France follows Italy but with a lower mortality a priori …
– However, be careful, there are a lot of insufficient elements in the count: you have to compare what is comparable, which is difficult in the current state of available information. Among other possible elements of measurement bias: death outside hospitals (among others in nursing homes), Covid case of decompensation catalyst or case by pathological mechanism, etc.

3. Health system: hospital vision “resuscitation”
3.1. Hospitalizations
3,195 emergency visits yesterday for suspected Covid-19 (3,745 the day before)
40% were hospitalized and 4% were admitted directly to intensive care (these 2 percentages remain stable)
36k tests (32k the day before) in the laboratory, including 30% positive tests. The tests are starting to be available, congratulations to the different contributing energies, because they are the key to an effective strategy.
3.2. Resuscitation: the real challenge now and in the future
6,017 cases are in intensive care (+ 452 cases in 24 hours).
Breakdown of cases by age:
- 1% (80 people) are under 30,
- 34% are under 60,
- 60% are between 60 and 80 years old.
The median age of resuscitation patients is now 58 years (decrease in age because we will not be able to accept all cases in resuscitation, in case the prognostic scoring – Apache type or other – will not be favorable).
Our health authorities are accelerating the effort at national level: more than 9,000 beds in intensive care are available today against 5,000 at the start of the crisis. A downside, because it is necessary to reason locally and in terms of load / capacity: we have 2 epicenters already at a maximum level of saturation: Ile de France and Grand Est.
As I said yesterday, it would be preferable to limit transfers to the West from the IDF or the Grand Est, because they exhaust teams (4-5 people for a patient), and create NOW to Paris has a AMS resuscitation of 1,000 beds. You have to think ahead, because in a week it will probably no longer be possible to transfer patients to other regions.
This AMS of 1,000 resuscitation units can be single or two-headed (2 x 500 beds): Hôtel Dieu, Val de Grâce,… We do not have the capacity to build 2 hospitals with 1,000 beds in 15 days like the Chinese l ‘did in Wuhan (11 million inhabitants, a population equivalent to that of Ile de France), but we have existing structures to transform in wartime and proactively. We define the objective (1,000 intensive care beds, the estimated need in a week) and we quickly find the human and material resources (private clinics, etc.). In the absence of such measures, either it will be necessary to “sort” upstream (age, pre-existing pathology, etc.), or the search for regulated beds will be unmanageable (therefore loss of chance for the patient in the emergency room).
3.3. Deaths
83% of the deceased are over 70 years old.
At the national level, an excess mortality of 14% is observed in week 12. It is confirmed with 19% in week 13 (March 23rd to 29th).

3.4. To be continued
Three types of places are at major risk of epidemic spread:
1. Ehpad: 14,638 confirmed or possible cases
2. Prisons: cases exist and affect both prisoners (promiscuity: 70k prisoners for 60k places) and supervisors
3. places of religious gathering (see examples from South Korea, Malaysia, Iran, Israel, Colmar): these places must remain closed for the benefit of all.
4. Regional vision
Always the East-West gradient with an epicenter, the Ile de France.

D. World: the epicenter is gradually moving to the United States
With the contribution of Stéphane, companion from the start.
The reported cases are unreliable data because they are very dependent on the layout of the tests, but other things being equal, the trend is an important element of decision-making.
As you are in “over-information” mode, some elements of understanding:
1. In short
The West (Europe and USA) accounts for 80% of existing cases, new cases and deaths.
The United States is the first country affected in terms of diagnosed cases: 217k cases.
In Italy, there are the first signs of a slowdown in Lombardy and Veneto: the number of daily deaths has started to decrease in recent days.
In China, after 2 and a half months of strict confinement, the inhabitants of Wuhan will finally be “released” in 5 days and will be able to leave Hubei and join their families. As a security measure, they are not yet authorized to travel to Beijing, where precautionary measures remain maximum, even vis-à-vis the other Chinese provinces (with the exception of some border areas of the capital).
In Germany, acceleration of the number of deaths with a doubling time to 3 days (to watch).
Passenger air traffic has recorded its largest drop since September 11, 2001.
2. Incidence : 80k (77k yesterday)
Chronological vision:

By country (top 10) :
USA 27k (+ 3k)
Spain 8k (+ 0k)
Germany 7k (+ 1k)
Italy 5k (+ 0k)
England 4k (+ 0k)
Iran 3k (+0)
France, Turkey 2k
Russia, Brazil, Portugal, Canada, Netherlands, Belgium: 1k

It would seem that the slowdown is confirmed in Italy, which has been on a “plateau” for a few days.

By continent

3. Prevalence
750k confirmed cases currently under observation
Doubling time around 7 days (stable)
Geographical location: 82% in the West
Top 10 countries:
USA 229k
Italy 83k
Spain 75k
Germany 61k
France 41k
Iran and England 31k
Turkey 17k
Switzerland 14k
Netherlands 13k
By continent

4. Mortality
By country
Note that the tip of France is linked to the inclusion of 884 deaths in nursing homes recorded since the beginning and presented yesterday.
Thanks again to my three companions from the start (Dr Bachir Athmani, Mathieu Bouquet and Carole Gabay)Virus Preventions 4 W’s:
Wear a mask, Wash your hands, Watch out for sick people, Wait for new updates from covidminute.com !
Protect yourselves, and above all protect the most vulnerable!
Dr. Guillaume ZAGURY,
Specialist in Public Health and Health Innovations
Consultant at “Health Innovations”
HEC
In China for 20 years“All success is collective”, thanks to:
– the whole “Back Up” team (Mathieu Bousquet, Carole Gabay, Flavien, Marie, Laetitia, Anne-Sophie, …), without whom this project would not have been possible.
– all the “Medical” team (Dr Bachir Athmani, Dr Ibrahim Souare, Dr Taieb, Dr Viateur …) who allow this project to exist,
– all historical financial sponsors (Jerome, Benjamin Denis & B Square, Benoit Rossignol, Arnault Bricout) who work for “Citizen Actions”
If you feel like a patron or of partners to finance IT development, don’t hesitate to contact me (guillaume@covidminute.com).
Also, even if part of the team is based in Shanghai, do not hesitate to come and join us, because there is no shortage of work :-)If you want to find more analyses and infographics, follow our account at:Know the latest updates
Powered byMedicilline