A. Ile de France, the current epicenter of the epidemic in France: create a AMS of 1,000 intensive care beds today
1. On average 450 new requests for resuscitation beds per day on the territory (452 yesterday)
Conversely, there are few resuscitation trips for the hour, the average duration of assisted ventilation being evaluated at 2 to 3 weeks.

2. Our absorption capacity is exceeded in IDF and in the Grand Est
Even if some patients start to go out, the outflow will be insufficient to compensate for the entries, and this for at least 10-15 days (the peak is not in sight).
3. We exhaust the healthcare teams with time-consuming and costly transfers
Whether to the western regions or to Germany, these transfers are not sustainable over time, because these spaces will soon be affected by the wave.
This mediated transport, certainly useful in peacetime, is extremely exhausting for the medical teams: it is especially necessary to mobilize 5 people to transport a stretcher.
36 patients were transferred out of Île-de-France by TGV this Wednesday to the Brittany region.
142 seriously ill patients from the Grand Est region were transferred abroad (Germany, Switzerland, Luxembourg).
To unclog hospitals in the Grand Est region, 18 patients in serious condition will be transferred by plane to hospitals in Toulouse and Montauban.
The means deployed (helicopters, trains, SMUR, etc.), even if they come from a commendable intention, are disproportionate and could be used to set up AMS-type structures “COVID”.
4. The only “wartime” solution in IDF: act immediately to anticipate the wave of the days to come and create a “AMS COVID” structure (Advanced medical station oriented towards resuscitation)
We propose to create a dedicated unit of 1,000 intensive care beds in order to anticipate the flows of patients in intensive care in IDF: advanced medical post of 1,000 intensive care beds.
Transfer to other beds in France will become impossible in the long term.
Currently, regulators are running out of trying to find places for a transfer from an emergency department to resuscitation beds dispersed in IDF. These steps take 2 to 3 hours and can have a life-threatening impact: in some cases, “every minute counts”.
We do not have the human and material means of the Chinese to build a new structure of this type. In 3 weeks, the Chinese were able to deploy 2 “Covid hospitals” of 1,000 beds each, with the support of 30,000 health professionals from all over China in Wuhan (city of 11 million inhabitants, the population of the Ile de France), and this was decisive and completely changed the epidemic shape of the curve, in particular allowing the cases to be isolated.
Faced with the short-term saturation of the current system, we must transform an existing structure into a AMS Covid of 1,000 intensive care beds (one of 1,000 or two of 500 each):
– it is necessary to centralize the resuscitation offer, so that transfers are fluid
– the objective may seem disproportionate “technically” and probably can cause an uproar (human and technical resources “impossible to find” … in peacetime!)
– but we are in time of war and all the active forces can and must be called upon on the objective (which is an order of magnitude to anticipate the evolution of the figures in IDF).
We don’t react to the epidemic advance, we anticipate it.
5. Physical location
In Paris a priori, and spaces are to be sought: Hôtel Dieu or other.
6. Be proactive and no longer suffer
Currently, we do not react to the epidemic advance, but we must now have a strategy to anticipate it (see Germany in Berlin or Russia in Moscow).
Given our current means (which certainly should improve but are still insufficient):
1. We orient our means of prevention towards professionals and at-risk populations (the situation is extremely distressing for these elderly people already often in a situation of isolation!)
2. The patient flow in acute respiratory failure is managed either on resuscitation (by available technical platforms), or in accompanying “palliative care” (physical and mental).
Otherwise, with the current dynamic, the health crisis of the heat wave of 2003 (15,000 deaths) risks being largely overcome.
Given that many journalists and decision-makers read us, I am sure that this preview message will be quickly taken up and relayed.
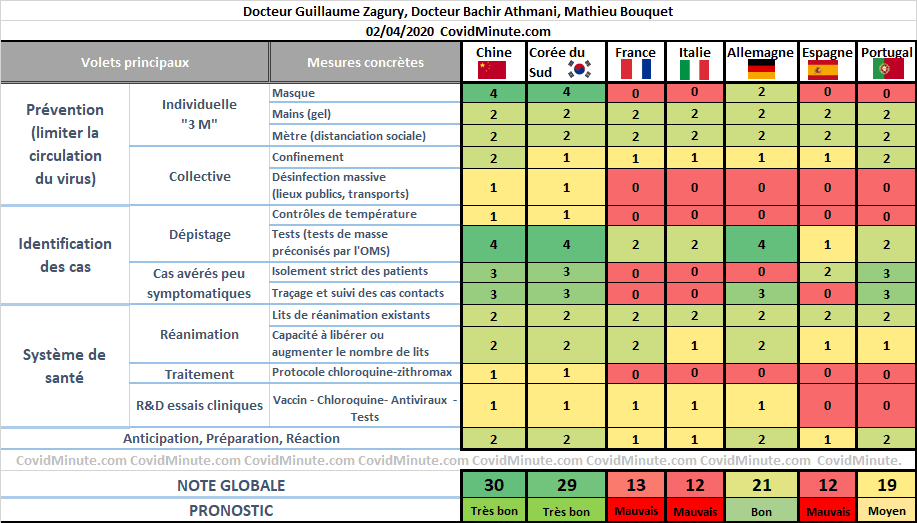
B. Measure the global responses of countries using our exclusive “Covid-score” table

Our “Covid-score” indicator assesses the measures taken in a country to reduce the risk of mortality.
This section is produced with discussions with Dr Bachir Athmani in Paris and Mathieu Bouquet in China.
1. Discrepancy between public discourse and reality on the ground: let’s change our peacetime discourse
Masks (and other protective equipment), tests, drugs (e.g. curare for ventilation management): many professionals have been waiting for more than a month. We will not need these materials in 6 months, but immediately.
We are in wartime, and must not depend on the outside: we know our Chinese friends, capable of redirecting “on the tarmac” an order of masks for a higher bidder!
What we see in France is often an answer:
1. with our values “in peacetime”: right to demonstrate maintained during an epidemic, use of electronic data considered too liberticidal, cumbersome administrative procedures (medical experiments according to time-consuming and unsuitable processes), etc.
2. giving the impression of “undergoing the match” permanently (compared to some other models: South Korea and Germany, among others). “We are growing in strength” is not the order of the day, we must now be 2 times ahead of the virus (hence our proposal above for example).
2. “If you can’t measure it, you can’t manage it”
To get things done, you must not procrastinate, even if you point your finger where it hurts.
Our Covid-score tool aims to contribute to this. Presented visually, this table is there for action: our decision-makers to use it.
3. Three main lines of action known for 3 months
The response to the spread of the virus generally consists of 3 parts:
1. prevention
2. identification
3. medicalization (treatment)
Each of these 3 components is divided into several measures, which we have identified in the form of 13 main actions (rows of our table), to which we add the anticipation, preparation and reaction measures demonstrated by the countries.
All the actions do not have the same weight and the same effectiveness, our team therefore assigned them a weighting element evaluating the impact of the measure, based on the results observed in the different countries affected by the epidemic, some countries Asians with more than 2 months of experience and perspective.
4. Today: comparison Spain (late measurements) / Portugal (early measurements)
The table includes a new country, Portugal.
5. Tomorrow: standard reference figures
The success standards are known (we have experienced it in Asia): we will provide the benchmarks tomorrow.
C. France D17
Analysis with the contribution of Dr Bachir Athmani and Jonathan Taieb.
The elements below are to be read with the reservations concerning the validity of the data (case definition, possible underestimation, etc.) already mentioned above, and keeping in mind that it is the trends that count, rather than the raw figures taken at time t.
1. Figures
56,989 confirmed cases cumulated by PCR tests (+ 4,861 in 24 hours).
24,639 hospitalized cases (+ 1,882 cases in 24 hours).
717 resource health establishments
10,935 recovered people have been discharged from hospital since March 1st.
4,032 people died in hospitals (+ 509 people): patients who died in nursing homes will soon be included in the figures (thus 500 in the ⅔ of nursing homes in the Grand Est), which will make it possible to become aware of the epidemic reality and to act accordingly.
2. Evolutionary dynamics compared to Italy
Number of cases (knowing that these data are highly questionable and depending on the number of tests available).

The absorption curve for resuscitation cases is more relevant.

3. Health system: hospital vision “resuscitation”
3,745 emergency department visits yesterday for suspected Covid-19, 38% were hospitalized and 4% were admitted directly to intensive care
1,328 interventions by SOS Doctor on suspicion of Covid-19
32,000 laboratory tests, 30% of which were positive yesterday.
6,017 cases are in intensive care (+ 452 cases in 24 hours).
80 people hospitalized in intensive care are less than 30 years old.
34% are under 60, 60% are between 60 and 80.
The median age of resuscitation patients is now 58 years (decrease in age because we will not be able to accept all cases in resuscitation because the prognostic scoring will not be favorable).
4. Regional vision
Always the East West gradient with an epicenter, the Ile de France.
In the French Territories DOM-TOM, there are 167 hospitalizations including 36 in intensive care, 85 return home and 11 deaths to date.

D. WORLD
With the contribution of Stéphane, companion from the start.
The reported cases are unreliable data as they are very dependent on the layout of the tests, but other things being equal, the trend is an important element in decision-making.
As you are in “over-information” mode, some elements of understanding:
1. Global vision
1.1. Incidence: 74k

1.2. Prevalence
635k confirmed cases currently under observation
Doubling time around 7 days (stable)

2. Chronological vision

3. Geographic vision
3.1. 80% in the West
New cases: 80% of new cases are in Europe and North America

Existing cases: 82% of existing cases (declared!) Are in Europe and America.
In Western Europe, 15k people were healed yesterday.

3.2. Top 10 countries: prevalence and incidence
USA 24k (+ 3k)
Spain 8k (+ 0k)
Germany 6k (+1)
France 5k (-3k)
Italy 5k (+ 1k)
Iran and England 3-4k
Brazil, Portugal, Canada, Turkey, Netherlands, Belgium: 1k

4. Analytic
4.1. In Italy
80,572 positive cases in Italy (+2,937)
13,155 deaths linked to Covid-19 (+ 727 deaths in 24 hours)
16,847 people recovered from Covid-19 (+ 1,118 in 24 hours)
To date, 110,574 people have been affected by Covid-19 to date in Italy.
4.2. In Spain
102,136 cumulative cases in Spain including 9,053 deaths (+ 864 in 24 hours).
2nd most affected country in terms of death
4.3. In United Kingdom
29,842 confirmed cases including 2,356 deaths (+ 183 deaths)
4.4. In Germany
74,508 confirmed cases in Germany including 821 deaths (+ 141 deaths)
Extension of confinement until April 16th.
4.5. In the USA
190,740 (+ 15,673) cumulative confirmed cases including 4,127 deaths (+712)
1st country most affected in number of cumulative AND existing cases
President Trump mentions between 100 and 200,000 victims as a target for health authorities.
The power of American medical research is focused on the goal of finding a technical medical solution to this crisis. And we know the capabilities of America in those moments.
4.6. In China
82,361 cumulative confirmed cases including 3,316 deaths.
4.7. In the rest of the world
180 countries affected
887,067 cumulative confirmed cases, including 44,264 deaths
185,541 people healed
Comprehensive “analytical” table and 2 digits after the decimal point, used by our Data Manager Carole Gabay:

E. Tomorrow
We will study medical advances in terms of technological solutions and in particular the prospects for serotherapy (passive immunity used for more than 50 years in particular for tetanus) from the plasma of cured patients, and from trials that are underway in the USA.
Thanks again to my three companions from the start (Dr Bachir Athmani, Mathieu Bouquet and Carole Gabay)Virus Preventions 4 W’s:
Wear a mask, Wash your hands, Watch out for sick people, Wait for new updates from covidminute.com !
Protect yourselves, and above all protect the most vulnerable!
Dr. Guillaume ZAGURY,
Specialist in Public Health and Health Innovations
Consultant at “Health Innovations”
HEC
In China for 20 years“All success is collective”, thanks to:
– the whole “Back Up” team (Mathieu Bousquet, Carole Gabay, Flavien, Marie, Laetitia, Anne-Sophie, …), without whom this project would not have been possible.
– all the “Medical” team (Dr Bachir Athmani, Dr Ibrahim Souare, Dr Taieb, Dr Viateur …) who allow this project to exist,
– all historical financial sponsors (Jerome, Benjamin Denis & B Square, Benoit Rossignol, Arnault Bricout) who work for “Citizen Actions”
If you feel like a patron or of partners to finance IT development, don’t hesitate to contact me (guillaume@covidminute.com).
Also, even if part of the team is based in Shanghai, do not hesitate to come and join us, because there is no shortage of work :-)If you want to find more analyses and infographics, follow our account at:Know the latest updates
Powered byMedicilline