
France comparison of the level of preparation (individual & collective) between April 1, 2020 and September 1 (Covid Score indicator created on April 1, 2020 – Dr Zagury & Athmani).
6 good objective reasons to be optimistic:
1 & 2) Epidemiological:
- The vast majority of children are spared
- In more than 98% of cases an adult will be cured.
3) Public Health treatments are known and now well available (strategy: “3M3T” – Hand Meter Mask at individual level & Test-Tracking – Triage (isolation) at collective level. This is illustrated by the Covidscore figure above with huge progress in the space of 5 months.
4) Our healthcare system, which “absorbed the wave” in April, has a proven track record and is not just in time.
5) Therapeutic solutions in perspective: More than 6 phase III clinical trials are underway and many virologists are optimistic about a favorable outcome (relatively stable virus)
6) The viral ecosystem is better and better known (fundamental knowledge: animal and human)

——————-
« All success is collective and I would like to involve the entire Medical team (of course Dr. Bachir Athmani, accomplice for 20 years, Dr. Mohamed Fadel, Dr. Marc Abecassis,….), the Datas Analysis team (Carole Gabay as lead, Laetitia Bernard-Granger,…), the IT team (Richard Coffre our excellent webmaster, Flavien Palero,…).
The CovidMinute team has been offering analysis on Covid19 since January 28. Your support is essential to continue to maintain our team. Thank you for your support.
Also, if you want to become a personal partner (geographic or technical or other,….), or institutional (so that we can acquire mapping tools for example), do not hesitate to contact me: guillaumez888@hotmail.com
For those who would be interested in a content delivery partnership (Academics, Media, Societies,…), know that we have been building BDDs since 28/1, with data (medical, public health strategies,…), which you will not find anywhere else.
—-ANALYSIS MINUTE —-
A / WORLD DYNAMICS: 30M cumulative cases declared & 830K deaths in 8 months.
A.1 / CHRONOLOGICAL ASPECT:
Stabilization of declared cases (= Dependent test => nearly 250 k / day), and declared mortality still at +/- 5 k deaths per day (5,900 yesterday)
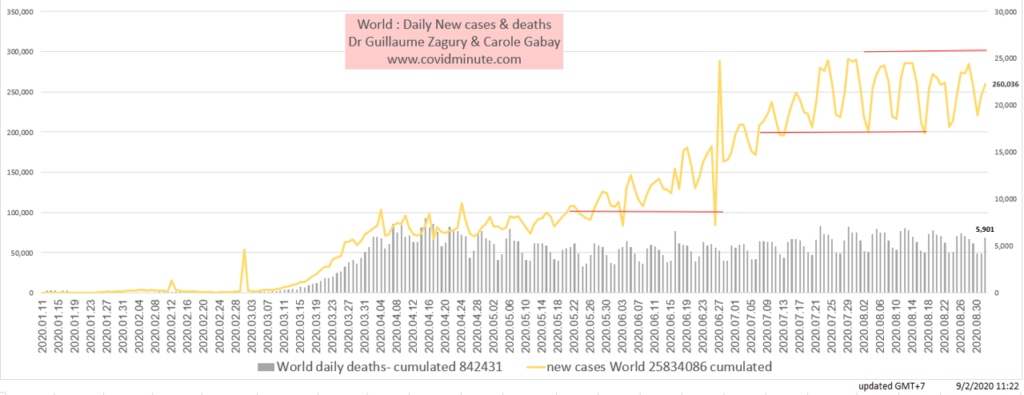
Note 2 points:
The observed “saw-tooth” aspect of mortality, with weekly recurrence, which should probably be explained by a less assiduous declaration / reporting process on the WE …
The preventive dynamic: because we test more and more (++), and more and more young (average age 39 years in Italy!)
A.2 / GEOGRAPHICAL ASPECT: 2 OR or 2 AND?
More than 100 “Wuhans” in the world, and let us note that Mainland China is the space which is the most spared in the world … and for good reason: fierce restrictions at the borders (thus in France it is 2 OR … in China it is 2 ET: Test before – Test arrival – Quarantine), adherence and total respect for barrier gestures, technological solutions (certainly potentially liberticidal!) used as much as possible for the benefit of Public Health…. This has allowed Mainland China to persevere in its objective of remaining a quasi “Covid Free” country for 4 months (less than 50 new cases / day and especially imported cases).
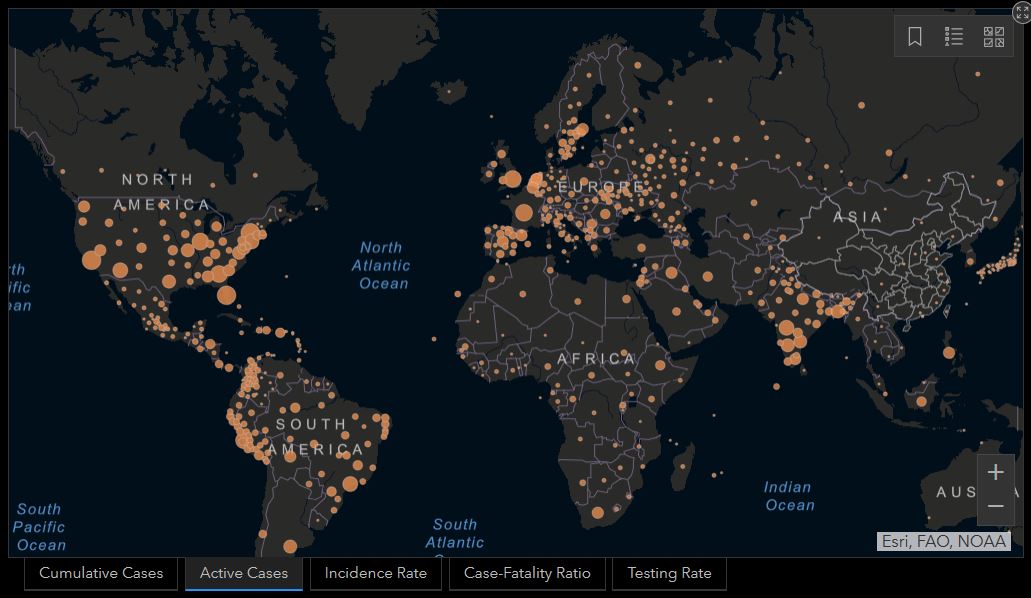
Source John Hopkins University
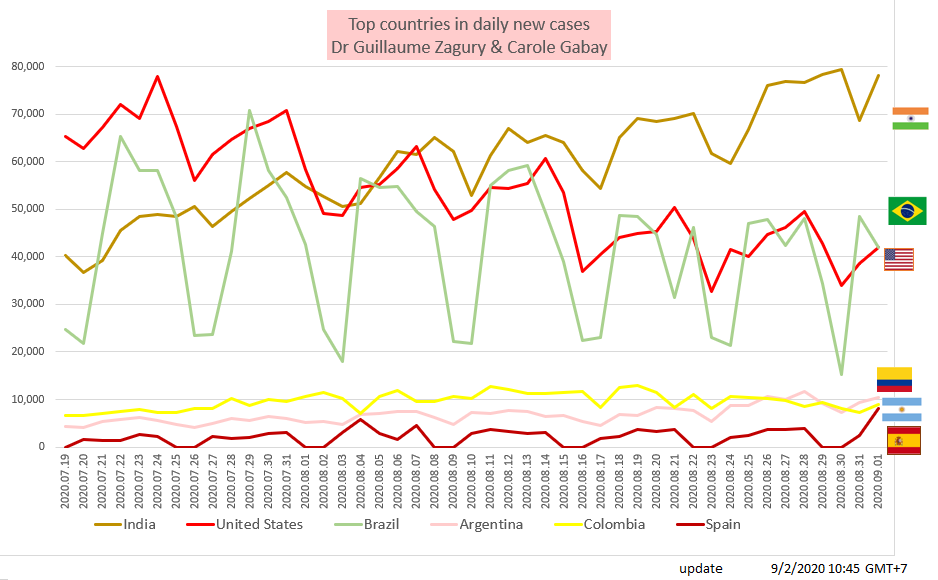
A.3 / WORLD INCIDENCE – 3 CURRENT EPICENTERS & THE INDIAN PHASE IS CONFIRMED
As expected for 3 weeks, India is in the epidemic phase (under declaration ++, but fortunately a “young” country & therefore to our knowledge: “Resuscitations are not full” …). The Americas still represent 50% of new cases reported on the planet.
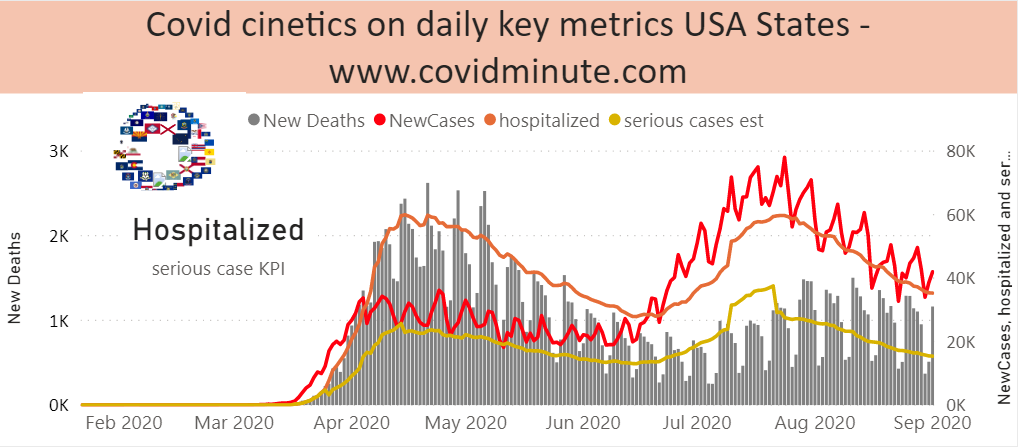
A.4 / PREVALENCE C + WORLD: USA & BRAZIL POSSIBLY IN “POST PEAK”(C +, ICU, DEATH)

Attention, the vision of the epidemic that with a “test” indicator is extremely questionable (+++), and therefore I invite you to see, the “country” figures using the 3 indicators having the most meaning: Hospitalization (when available!) -ICU (when available!) – Death
A.5 / AMERICAS FOCUS: SLIGHT IMPROVEMENT
for the 2 most affected countries on the planet: USA (182k deaths) & Brazil (116k deaths)
A.5.1 / USA: SIGNIFICANT IMPROVEMENT
(Hospitalizations and ICU down), but VIGILANCE anyway (still 1200 deaths yesterday, … but it was a Monday and we know they represent the situation at S-2) …
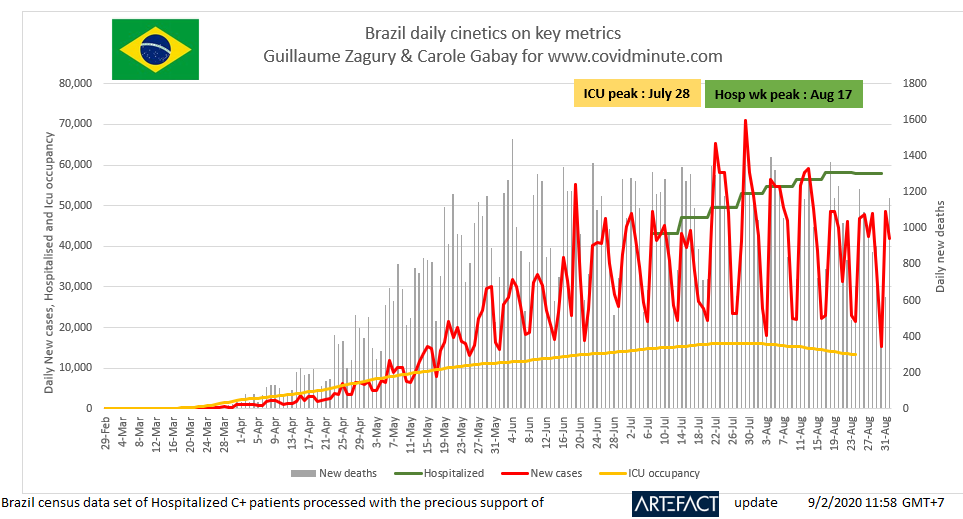
A.5.2 / BRAZIL:
Brazil on a rather favorable plateau (slight drop in ICU, slight increase in Hospitalizations, and a number of declared daily deaths hovering around 1000)
This excellent graph made with Carole Gabay allows to visualize the evolutionary trend
A.5.3 / INDIA: IN THE EPIDEMIC PHASE
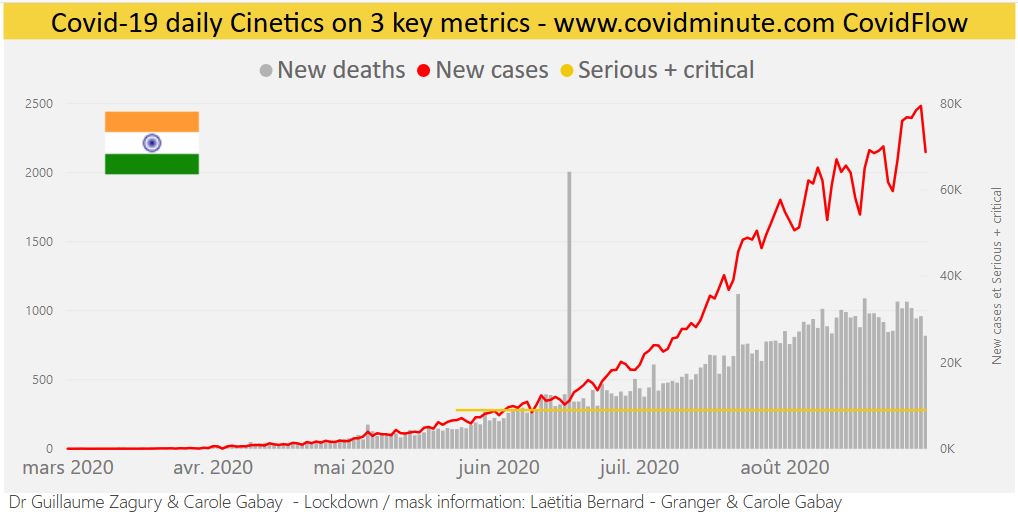
Obviously, a continent country with underreporting (and difficulty in aggregating data), but the country’s youth, hopefully a good omen, for this continent country (1.4 billion inhabitants)
A.6 / GLOBAL IMPACT: DEATH ANALYSIS
A.6.1 / The West for more than 90% of declared deaths (830 K to M8):
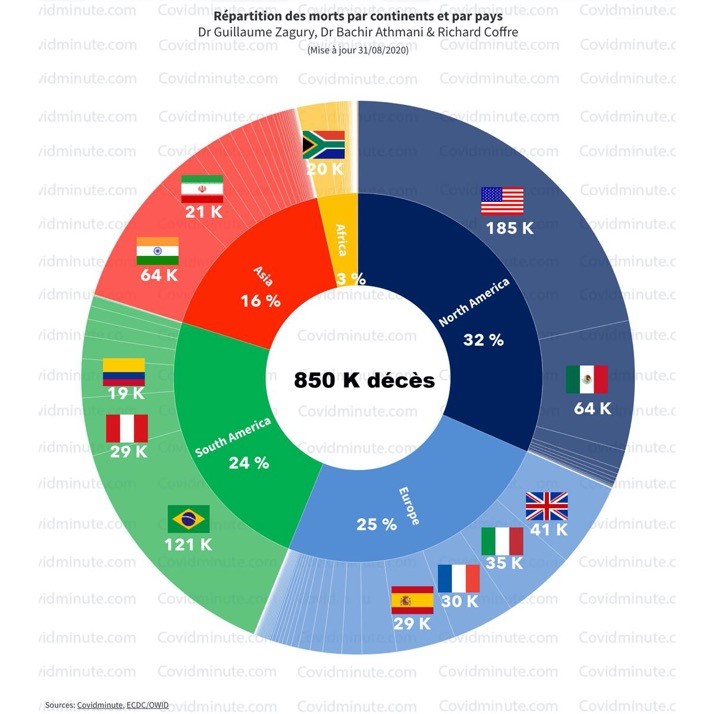
This graphic innovation makes it possible to visualize both Continent and Country information.
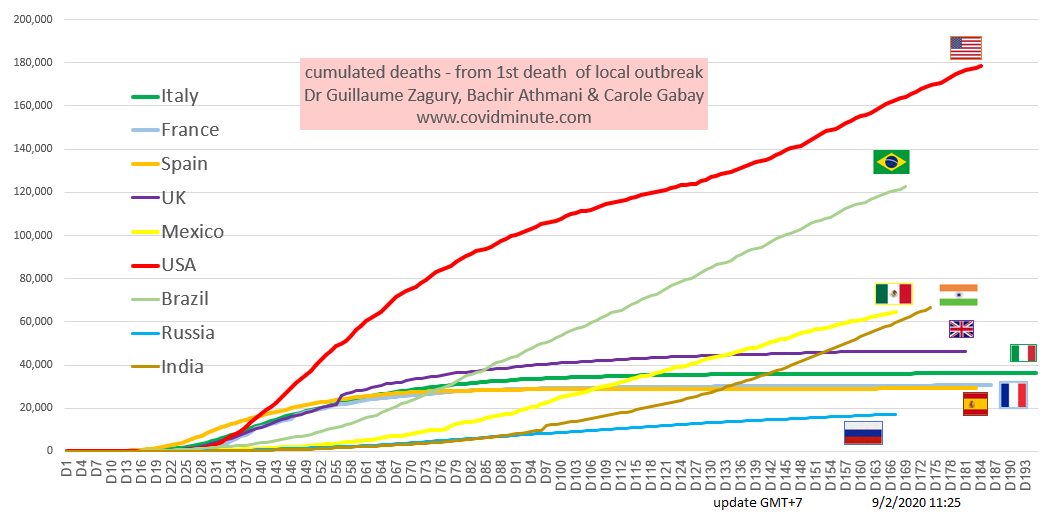
A.6.2 / TOP 10 COUNTRIES:
Chronological evolution of deaths by country: The Americas above all (3 first countries affected and India in the active phase)
A.6.3 / RESULTS INDICATOR:
Watch out for shortcuts….

This indicator is interesting if we compare “apples to apples”, which means “homogeneous” definition of the numerator (“Covid death”), and even epidemic environment for interpretation.
A.6.4 / NO PERFECT OBJECTIVO-SUBJECTIVE PARRALLELISM (FEELING OF THE POPULATIONS)
Note the lack of perfect agreement between the “objective” aspect (death / M) of the result and the subjective perception of the population (survey: Pew Research Center – USA): case of Japan (good result – low bar – but felt popular low efficiency!)
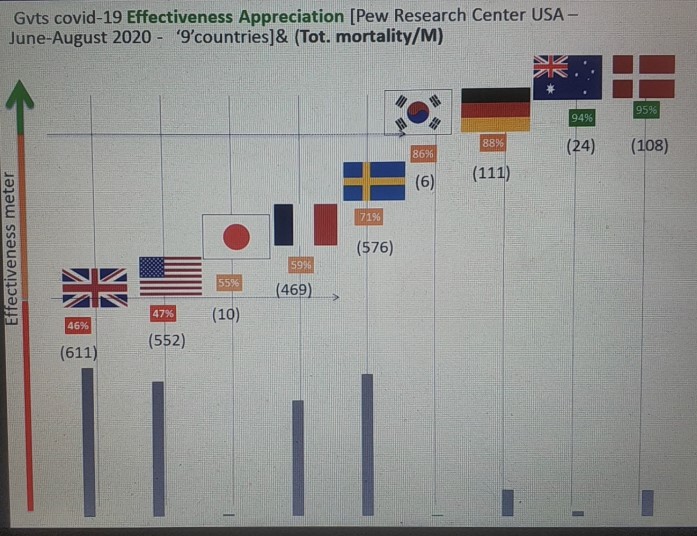
Next week, we will illustrate our point with a reading: “Belgium”.
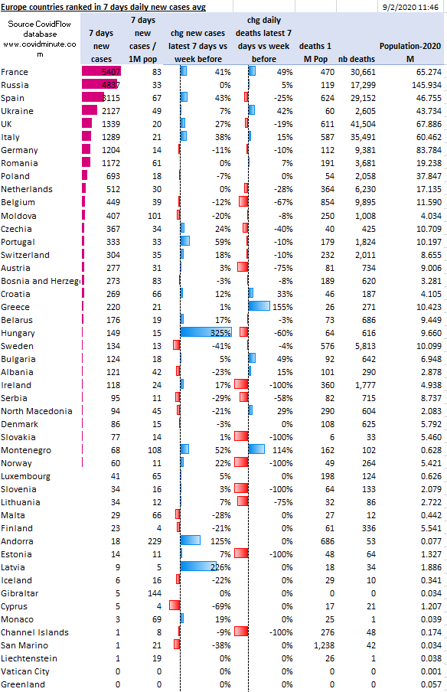
B / EUROPE: A EUROPE OF REGIONS
B.1 / GRAPHIC VISION: RELATIVELY POSITIVE situation
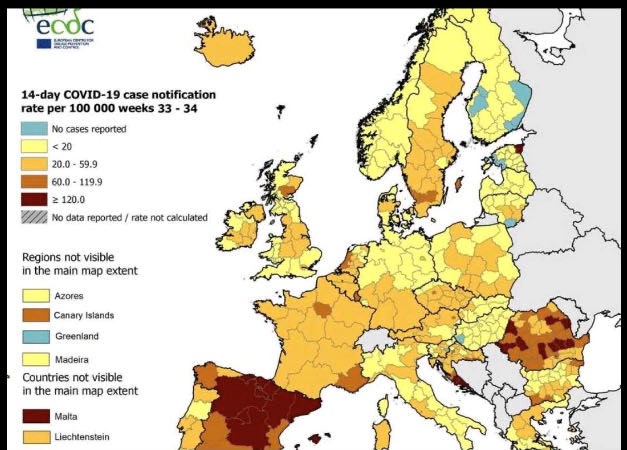
European Center for Prevention
B.2 / DETAILED VISION:… but WITH VARIABLE GEOMETRY AT NATIONAL LEVEL: France, Spain, Ukraine…
C / FRANCE: civic attitude: The parents of the young C (+) of today can be the hospitalized of tomorrow …
As in economics, there are many indicators (Hospitalizations, ICU cases, Deaths, test positivity rate, C + incidence, R0 index, SOS C + calls, etc.), which most often come together to identify a trend. No indicator is perfect, and each measures part of the problem. I particularly recommend the first 4, which reflect an indisputable “field” medical reality and the speed of circulation of the virus.
However, knowing that we can make figures say a lot of things, when they are not relativized in time, and in space: thus a simple recent C + curve, can give the impression of an “alarmist” epidemic rebound, whereas the Hospitals hardly register any new patients!
C.1 / WE TEST MORE
(around 150 k / day), but the situation cannot be compared to April: as a result more C + declared (and much younger – cf. tests in April)
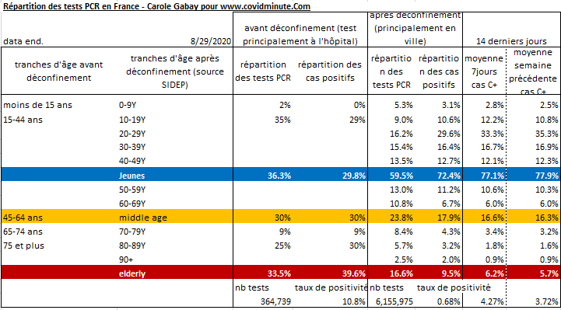
For the tests: it is not only the quantity of the tests that is important but the quality and at several levels:
the sample itself (false positives and false negatives).
targeted test (sick, suspects, contact cases) => Separate these sampling sites from those who are tested for a trip or out of envy (to avoid infecting everyone).
keep in mind the objective of the tests: diagnosis to isolate (sort) and trace
put the family doctor back at the center of the process: thanks to his national network and his knowledge of the field and of the family …
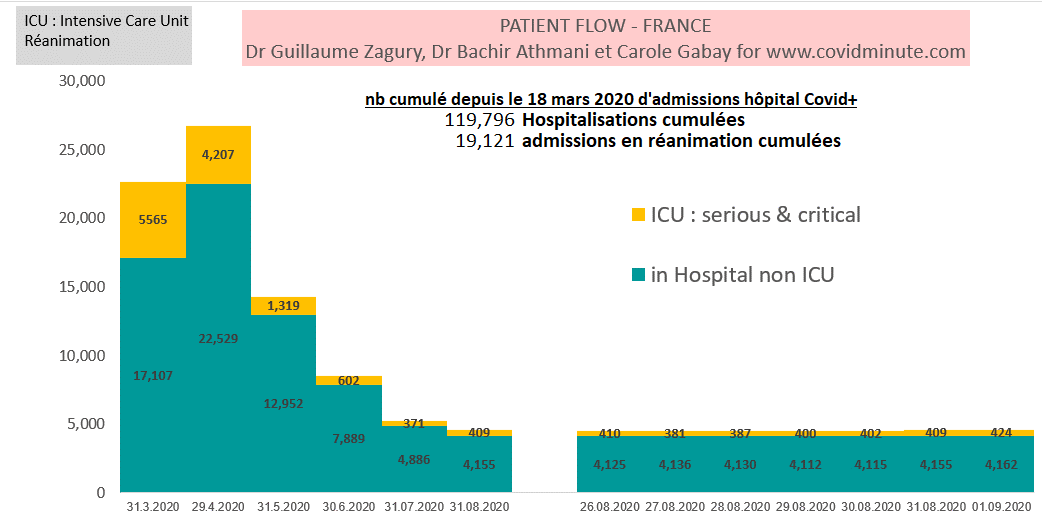
C.2 / THE SITUATION CANNOT BE COMPARED TO APRIL:
C + hospitalizations (with ICU): 4400 (or roughly 6 times less C + / April)
ICU: 424 (versus 409 last week)
Deaths: 24 (versus 15 last week)
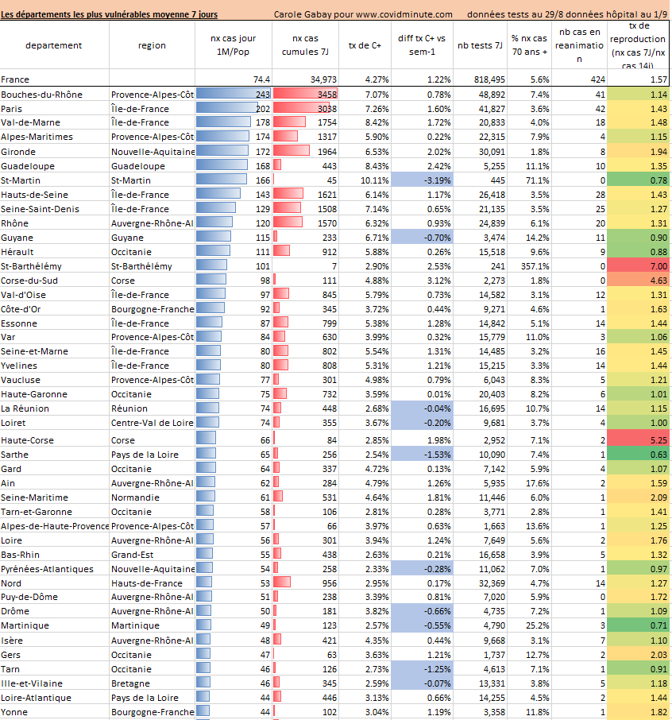
C.3 / We must reason at the LOCAL level:
Vigilance in IDF & PACA
But do not be naive and do not let the “embers become fire” with the returns and re-entry: maintain individual vigilance (“3M”)
The virus is circulating (around 3000C + / day currently) at different speeds depending on the region: more than 700 “Clusters”, and 3 regions to follow: IDF, PACA, Guyana…
Our “Department Barometer” (analytical innovation by Carole Gabay)
At the “micro” level, it is extremely difficult to establish clear actions of Public Health without being in a certain way liberticidal (cf. mask, test, isolation…) and the level of security varies according to the viral spread. . As this magnificent pharmaceutical observation says: “Between the drug and the poison, it is only a question of dosage”. Everyone must be responsible and adapt a citizen attitude of “mobile confinement = mask and intelligent = perception of a risky situation” …
D / GEOPATHOLOGY (section created in February!) – VACCINE: ALL VACCINES LEAD TO MAN (continued)!
-Different vaccine strategies are being evaluated, primarily targeting humoral immunity (antibody production), with different virus-based platforms (eg inactive, attenuated), viral vector-based (egadenovirus, measles) , nucleic acid-based (eg RNA or DNA), protein-based (eg vaccine subunit or vlp).
Even if qualitatively, the first vaccine available on the market will probably not be the best (number of injections required,% of effectiveness, iatrogenic risk in the short and medium term), the impact of its “announcement effect” will vary. mark the conscience in terms of “world technological leadership”, particularly in the match between the USA and China.
Taking into account the validation requirements according to international standards (FDA, CFDA, EU …), the Chinese inactive vaccine (low tech) developed by CNBG (China National Biotech Group), and having already been administered to 20,000 “volunteers” before d ‘be used abroad (Middle East, Morocco, Latin America), is probably the first that will be authorized at the international level (probably around the end of November), because if the genetic engineering projects (high technology) developed by the American Moderna or the Oxford team are relatively quick to implement for a phase 3, their validation will probably be slower because of the still unknown side effects inherent in this type of new vaccine. On the other hand, China’s influence at WHO is also a factor to be taken into account.
Concerning the temporality, 3 elements of reflection, on more than 100 vaccine candidates launched (often by international consortia), including 6 officially in phase 3 since July 15 (Africa, Brazil, Middle East,…).

Russian vaccine Sputnik V (accin)
Injection to 40,000 individuals next week, for phase 3 in Russia because the epidemic is still active (1 million cumulative cases). This will target, first of all health personnel because they are particularly exposed (we are talking about 200 deaths), then educational personnel (child contact, etc.). Note that if money may not be happiness, it does make volunteers (see phase 2, compensation of € 1,600, or 3 times the average salary). No international scientific publication to date and probable mass vaccination in January for the Russians, if the results are “convincing”.
-The “USA” vaccine: will the scientific tempo be respected or will it be an exceptional procedure for the FDA?
Stephen Hahn, the head of the United States Medicines Agency (FDA), has announced that it is possible that a future vaccine against the coronavirus will first be authorized in the United States under an emergency procedure, before the end clinical trials intended to confirm safety and efficacy. “It will be a decision based on science, medicine, data. It will not be a political decision, “he told the Financial Times very recently, denying that he was under pressure from President Donald Trump to authorize a vaccine before the November 3 presidential election.
-As my specialist friend Dimitri says: “The vaccine has no borders, but researchers have a nationality”
….To be continued
E / Deep Diving:
At all times, you can :
- download the materials developed since we started the www.covidminute.com journey on https://covidminute.com/visuels-memos
- peruse the complete decks of graphs / tables, which we update for each article https://eng.covidminute.com/charts/ – the decks for France and China are updated every day following the update periodicity of the sources.
- explore the CovidFlow interactive web pages which is updated twice a day for over 200 countries and 50 States of the USA. https://eng.covidminute.com/covid-flow/
————————————————————————–
As since February:

-The “3M”: for 70% of the population at very moderate risk
& I added Minute = limit prolonged contact: “4 M” for the 20% of French people over 65, the 10% of people at risk (roughly: cf. Long-term conditions) and the +/- 2 million caregivers particularly exposed….

Dr Guillaume ZAGURY,
Medecin Practitioner,
Specialist in Public Health and Medical Innovations
MBA
In China since 2000.
