
Dr. Guillaume Zagury, based in Shanghai, a specialist in international public health and health innovations, comments for the Community onthe evolution of the epidemic for more than three months, and provides a preview of the elements of understanding on its “country and regions analysis” and predictable consequences (experiments of SARS in 2003 and Covid-19 in China).
A remarkable multidisciplinary teamallows the realization of this analysis which is intended to be factual and objective (by the way, do not hesitate to join us: mail below):”anysuccess is collective”.”.
Beyond the volunteer skills, this project wasmade possible by the support of our citizens’ vision patrons: the Paul Bennetot Foundation (Matmut Foundation under the aegis of the Foundation of the Future), B Square, Tag Advisory, Daxue Consulting, as well as various companions (Jérôme, Dr BenoîtRossignol, Gilles Langourieux, Sabrina Rocca… )
All our illustrations created for more than 100 days, will soon be available on our website and you can download a large part of them. (www.covidminute.com).

I. COVID “360 MINUTE”: graphs and maps (80% of the information)

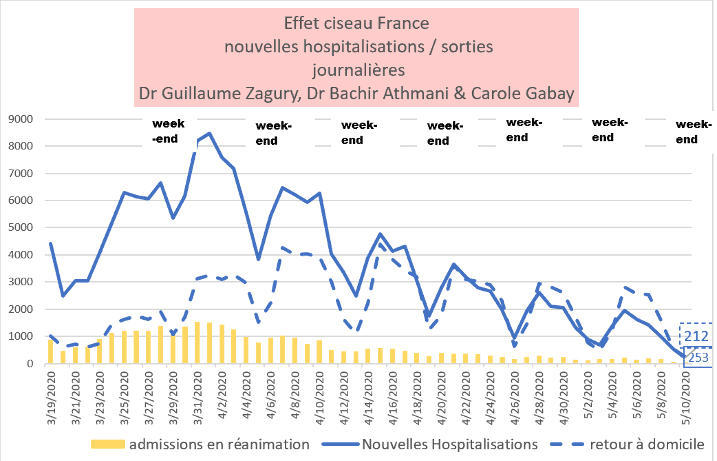
I.1 France – D. Day, a favorable dynamic (70 deaths yesterday – lowest death toll)
But slow: still 500 new hospitalizations per day despite 55 days of confinement.
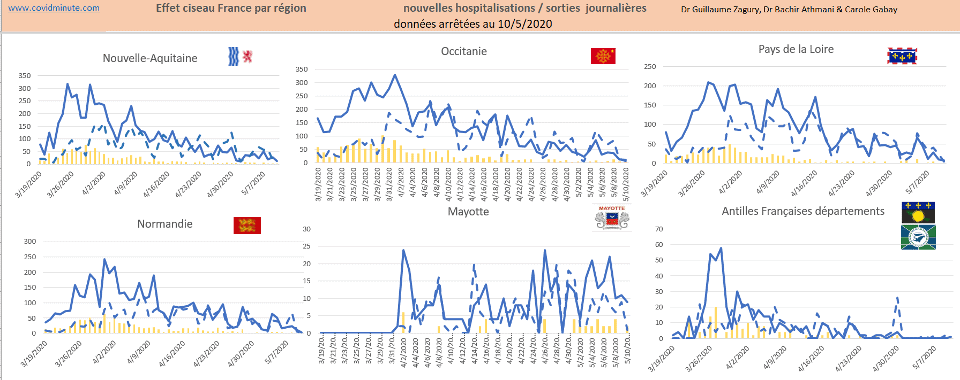
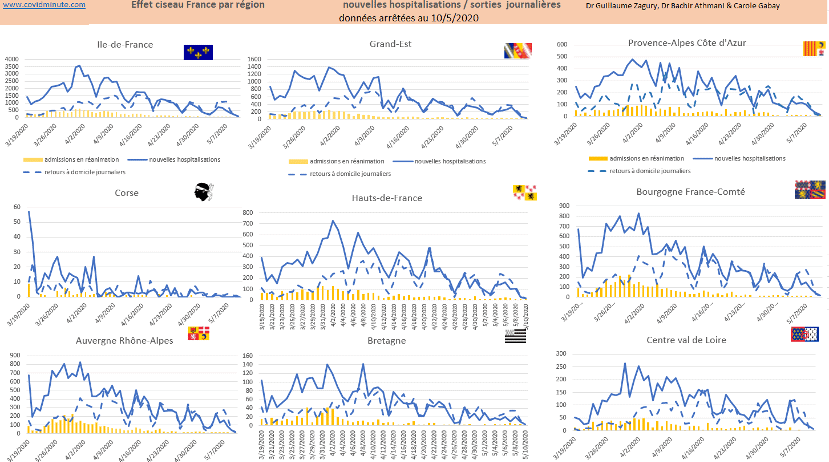
France: scissor effect in progress (Hospitalizations: more exits C- than entries C)
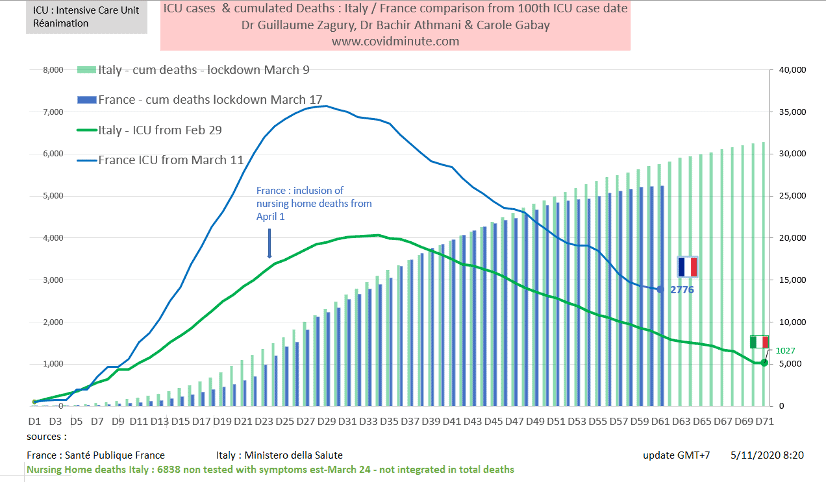
I.2 Vision time: we follow Italy with 10 days lag
Comparative chronological evolution of resuscitation cases France/Italy
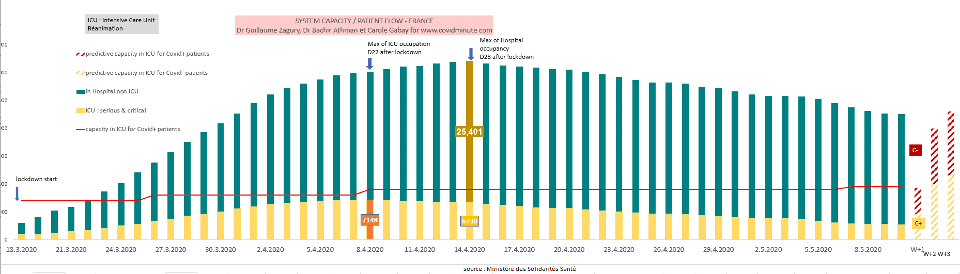
I.3 France – Forecast for deconfinement: resuscitation beds available – the issue from 16 May: the curative system will have a hard time with a “seconde vague” C ()withthe C (-) that will gradually return (possible tension from 16 May)

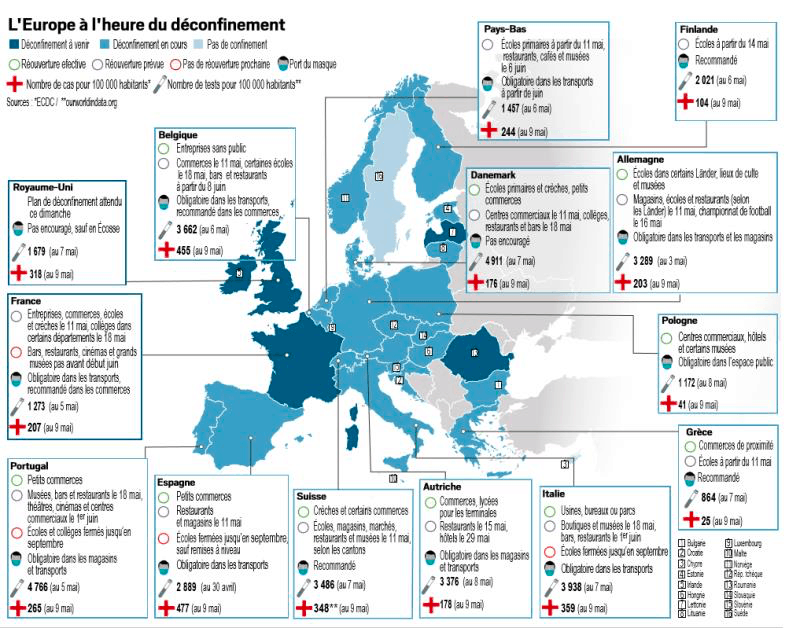
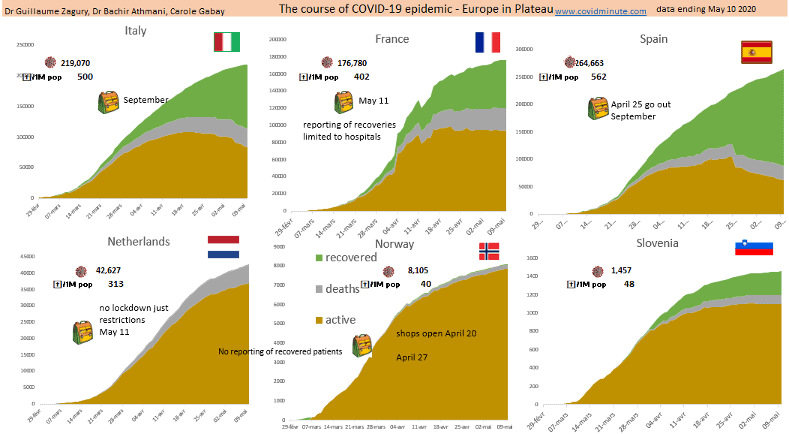
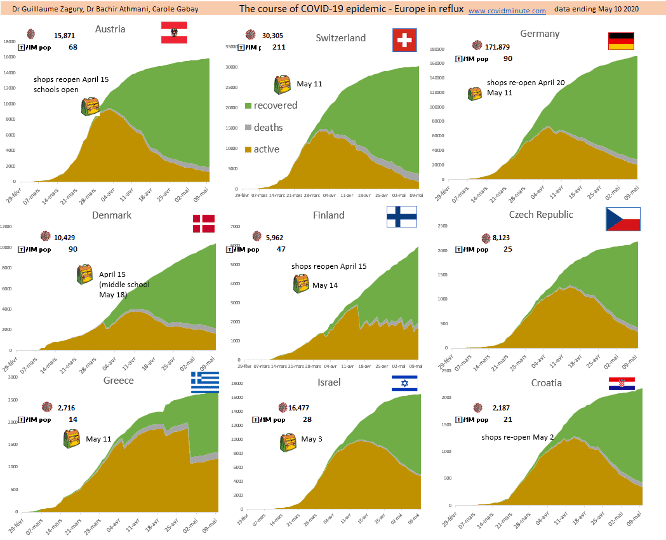
I.4 Europe: a 3-speed Europe: past peak (deconfinement) – plateau – epidemic phase.
Note that in France, Ehpad patients cured or non-hospitalized patients, are not counted in the “healed”, and as a result, the flex (importance of the “green”) of the curve is actually stronger than the “graph” vision.
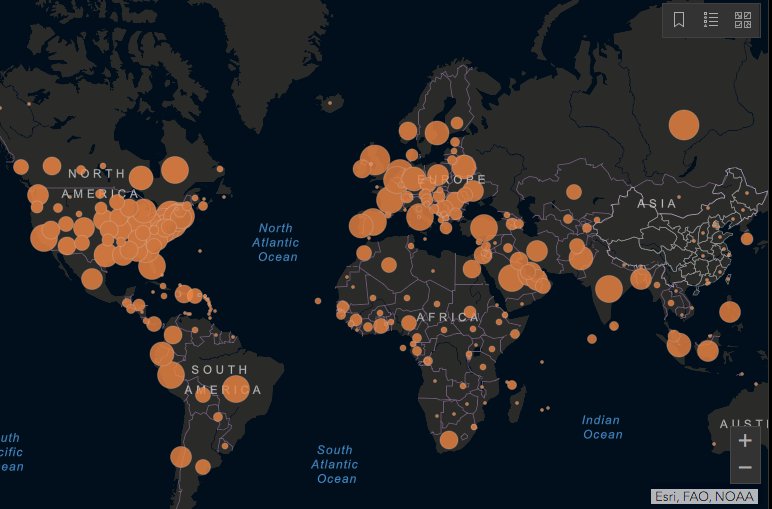
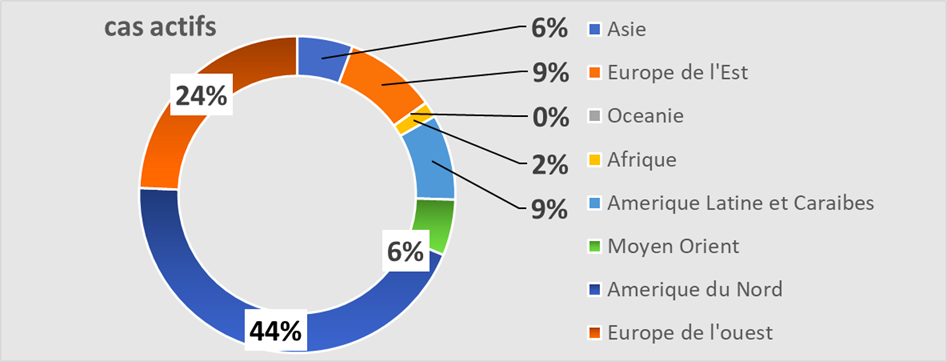
I.5 Epidemic Mapping (reported active cases): 5 active households (North America, Latin America, Europe, Middle East, Russia)and nearly 50 “Wuhan” Amérique
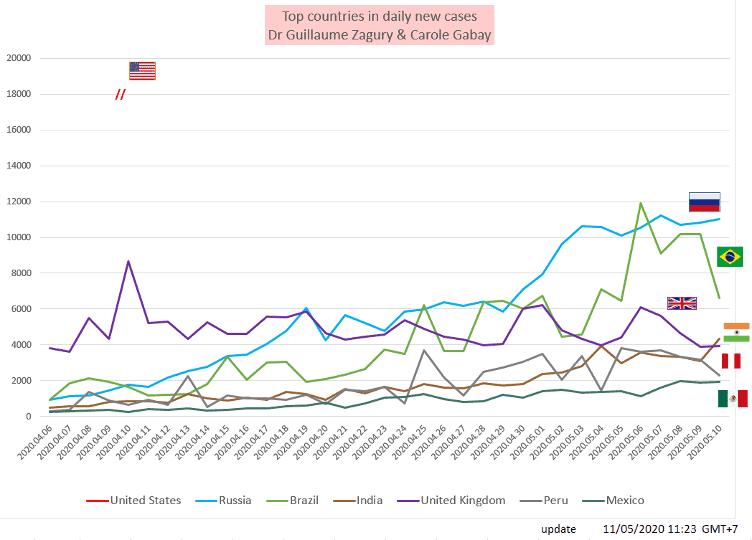
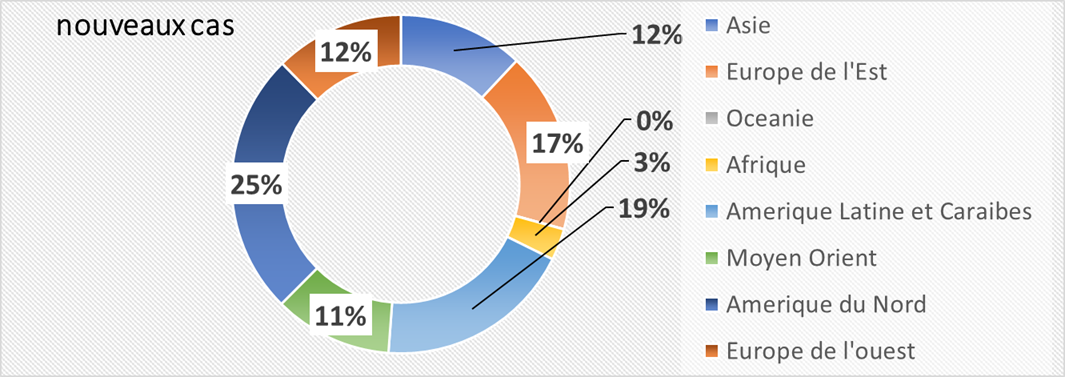
I.6 World: Latin America in epidemic phase with a number of new daily cases
Tending to reach the USA (with probable under-reporting …): 20% versus 30% of new cases reported (with the usual reserves on this type of dependent)

I.7 World – outcome indicator – mortality / 100k individuals: 3 levels observed
Comparative international results of “country strategies”
Indicator certainly not perfect (because of the tests, population density, the median age of the country …) but available, to assess the impact of “country” strategies.
Beware, however, of too hasty comparisons (see Finland or Australia to low population density versus Singapore or New York)

II. 360-degree analysis:
With the Collaboration of Dr. Bachir Athmani and Carole Gabay
Ⅱ. A Let’s Stay Modest: Scientific Time To Test Media Time
Ⅱ. A.1 Until now, children have been considered high sources of transmission
Underlying argument being the case of influenza
This was a strong argument for iron sea very quickly schools(cf in Asia and often in Europe)
Ⅱ. A.2 Current studies now run counter to this principle:
It turns out that carrying in children is equivalent to that of adults, in terms of viral load, but that thetransmissioncapacity would be low.
The case of the 2 children”contaminated with Contamines (!)” is an example: the two classes attended had shown no other positive cases.
Ⅱ. A.3 This is also true for many points where we observe a lack of consensus:
Examples include: seasonality of the virus, effect of temperature/humidity, host animal, clinical elements (e.g., anemia not observed in China… ), chloroquine efficacy, post-infection immunity (level of protection… ).
Ⅱ. A.4 A specificity of this pandemic is thus the media speed (following the rise of ICT and especially “Social Media”), which is upsetting the medical-scientific world
1/ Science needs time to establish a truth (via results found in time and space), but the context of “viral warfare” requires prioritizing all potential avenues.
2/ In this hyper-scientific global competition (“Soft Power concept”), 2 remarks:
- Diplomatic issue: China is becoming a major player in terms of the amount of scientific publications.
- Communication with certain races to therapeutic announcements, on the one hand to reassure the population, and on the other hand to find partners (technical, financial … )
Ⅱ. A.5 On a personal level: the over-information observed (for example: more than 5,000 Covid scientific papers in 4 months) is faster than the human ability to analyze it
This thus generates for decision-makers a “feeling of paralysis” following numerous contradictory data (“what was true yesterday is not necessarily true today”), and evolutionary (appearance of a new rupture therapy for example…).
In total, technological tools (NTIC and social media) allow for an acceleration of knowledge (“globalization of research”) and its dissemination, but also generate decision-making complexity through the over-information produced.
Ⅱ.B Europe
A west Es gradient- on the number of recorded deaths (May 9):
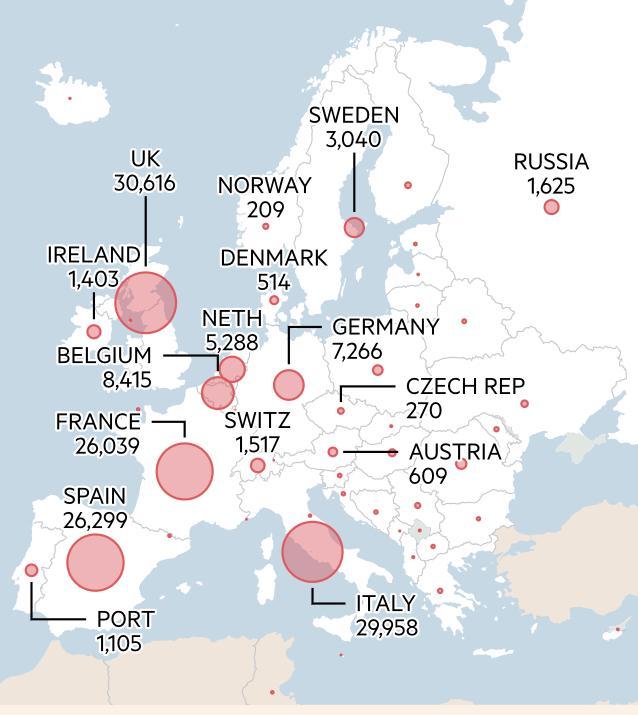
Countries that have deconfinated
Ⅱ. C France – J50 containment assessment:
Ⅱ. C.1 Scissor effect but still high plateau (500 new cases per day despite 55 days of containment): cf minute analysis
Ⅱ. C.2 Preparation for deconfinement – loco-regional vision: 2 gradients – East-West and North-South (27 departments still en red)
At the regional level: cases of hospitalizations
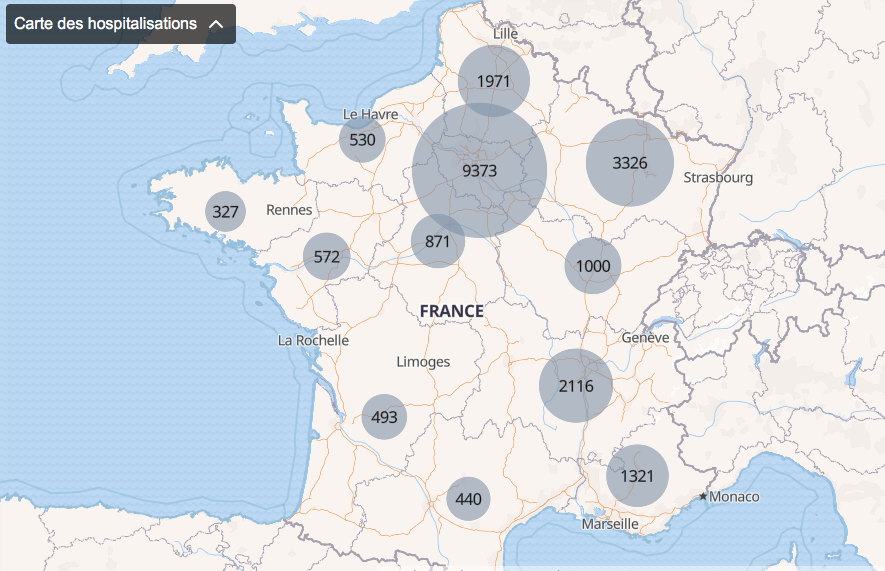
- Departmental vision of combinations of the two factors: case density and available resuscitation beds (red: 2 negative indicators – orange 1 indicator – green: 2 positive indicators)

Ⅱ. C.3 Preparation for Deconfinement: Regional Analysis: Resuscitations prepare:
Ⅱ. D WORLD: The 2 Americas and Russia in epidemic phase with about 20% of new cases
With the contribution of Dr. Bachir Athmani, Stéphane and Carole Gabay, companions of the first hour, whom I thank again for their unwavering support.
Beware of certain figures (number of cases, deaths…) that are highly questionable because they vary from country to country (e.g. availability of tests), with measurement biases and therefore major under-reporting in some countries.
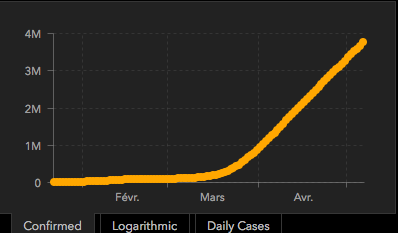
Ⅱ. D.1 Prevalence: 2,422,000 active cases confirmed for observation

Epidemic growth since January 1: about 4 million historical cumulative cases
Geographical vision: 5 households – North and South America, Europe, Middle East, Russia – iconography in minute analysis
By continent: The USA and Latin America (10% of current and probable cases underreporting): 54% of cases reportedworldwide
Top 10 countries: full country table (time /space) on: www.covidminute.com
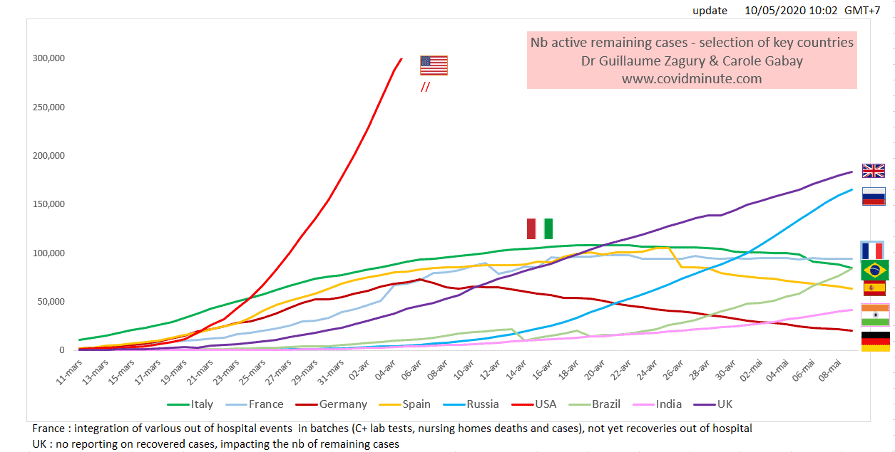
United States 1.04M (yesterday 1.03M)
United Kingdom 187k (yesterday 183k)
Russia 173k (yesterday 165k)
France 94k (yesterday 94k)
Brazil 90k (yesterday 86k): underestimated figure according to experts
Italy 83k (yesterday 85k)
Spain 62k (yesterday 63k)
Peru 44k (yesterday 43k)
India 44k (yesterday 41k)
Turkey 42k (yesterday 44k)
Netherlands 37k (yesterday 37k)
Ⅱ. D.2. Impact: 76,000 new cases detected yesterday

Depending on the weather:

Geographic:
By continent: Latin America and Russia also in epidemic phase
By country

By country
United States 18k (25k yesterday)
Russia 11k (11k yesterday)
Brazil 7k (10k yesterday)
United Kingdom 4k (4k yesterday)
India 4k (3kyesterday)
Peru 2k (3k yesterday)
Spain 2k (3k yesterday)
Pakistan, Singapore, Iran, Saudi Arabia, Qatar, United Arab Emirates, Kuwait, Bangladesh, Belarus, Ukraine, Turkey, Italy, Sweden, South Africa, Canada, Mexico, Chile: 1 to 2k
All the tables of our Data Analysis Expert, Carole Gabay, on the website: www.covidminute.com, in the “Resources” section.
III. TOMORROW
- What’s new in the US: cases in resuscitation, gross and relative mortality (graphic comparison)
Keep in mind the “3M reflex” (Hands-Masques-Meter) to protect yourself and “reflex 4M” (Hands-Masques-Meter-… Minute) for frail people (personnel caregiver)
… but above all to protect the most vulnerable.
Confidence and solidarity for this collective struggle
Dr Guillaume ZAGURY
- “Allsuccess is collective,”thanks to:
- The entire “Medical” team of “GCMN” type (Global Covid Medical Network): Dr. Bachir Athmani, Dr. Marc Abecassis, Dr. Mohamed Fadel, Dr. Jean Michel Serfaty, Dr. Ibrahim Souare, Dr Jonathan Taieb …) that allow this project to exist,
- The entire data analysis and IT team: Carole Gabay (“Data Analysis Expert”), Richard Coffre (exceptional webmaster), Flavien Palero (digital manager), Mathieu Bouquet (for his past contribution)
- The whole “Communication” team (Flavien Palero, Laetitia, Marie, Alison…): without whom this project would not have been possible.
- All the historical financial patrons (Jérôme, Benjamin Denis and the B Square Consulting Company, Benoit Rossignol, Arnaud Bricout and TAG Advisory and Gilles Langourieux, Sabrina Rocca…) who work for “Citizen Actions”
- Also thank us sthe PaulBenetot Foundation
- If you feel like a patron or partner to fund IT development (all the others have been volunteering for 88 days!), please contact me (guillaumez888@hotmail.com).
- Also, our team, although partly based in Shanghai, will be delighted to welcome you … because it’s not the work that’s missing…!
[DISPLAY_ULTIMATE_SOCIAL_ICONS]
