
I. COVID “360 MINUTE”

I.1 France – after 45 days of containment a favourable but slow dynamic
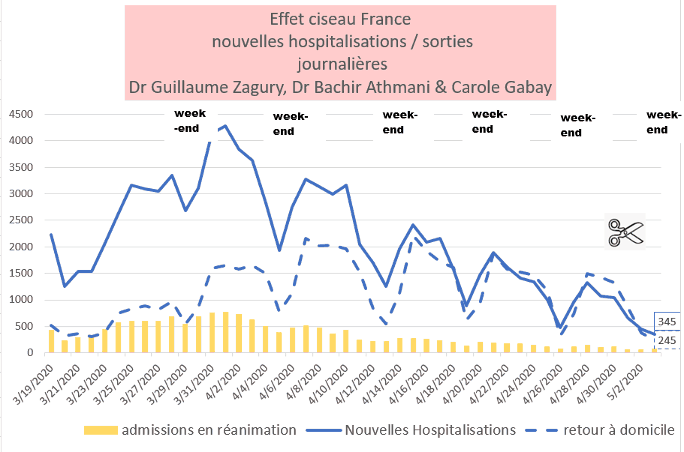
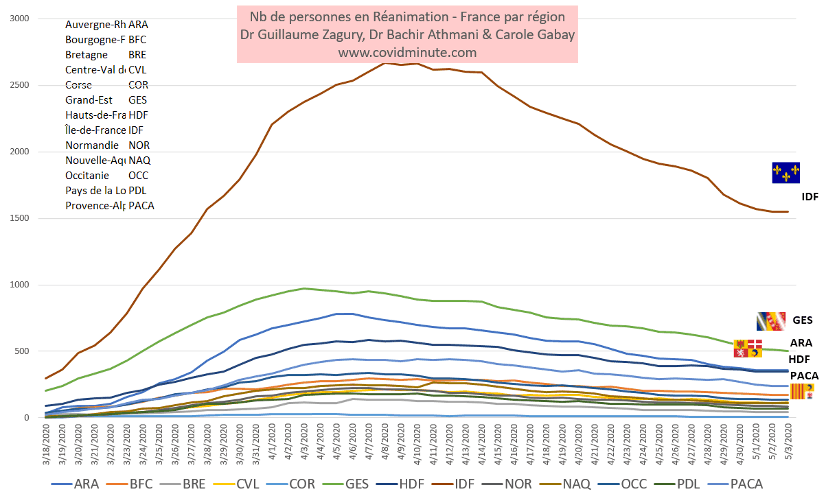
Scissor effect in progress (hospitalizations and resuscitation)
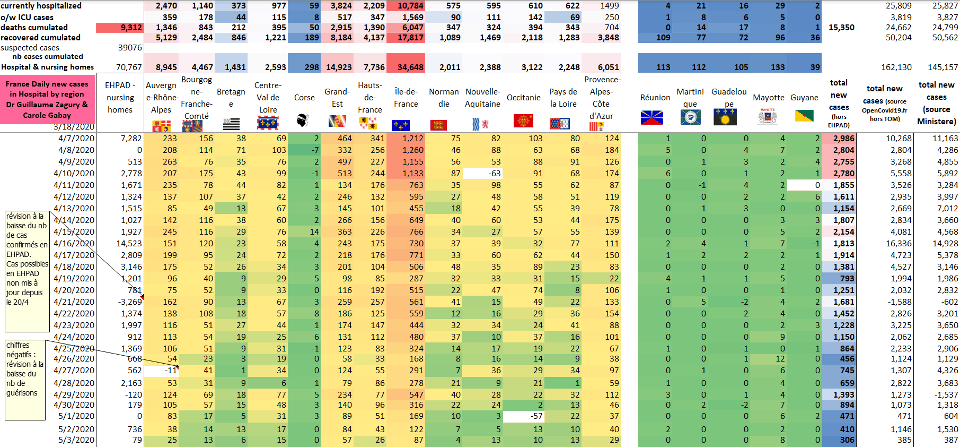
Fewer than 400 new cases in France
France: scissor effect in progress (Hospitalizations: more exits C- than entries C)
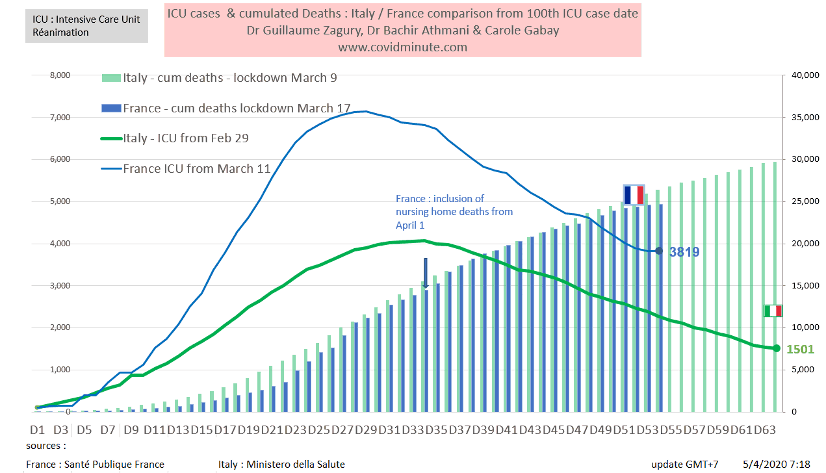
I.2 Vision time: we follow Italy with 10 days lag
Comparative chronological evolution of resuscitation cases France/Italy
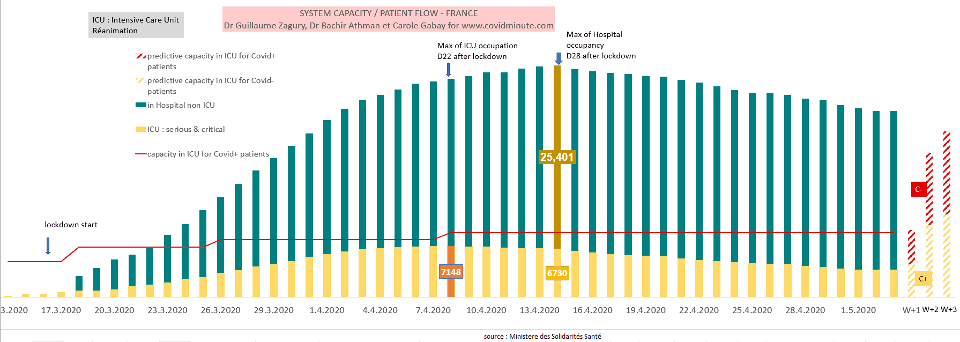
I.3 France – Forecast: resuscitation beds available (at stake from 16 May)
- The Cova beds () below 4000 today (3827 versus 3878 yesterday) with a maximum capacity to date estimated at 9000 beds.
- Post-de-disconfinement projection, based on 3 elements: historical data, incubation time (J7 with an upsurge expected around 16 May), and the influx of patients C (-) (3305 out of 7183 occupied beds)
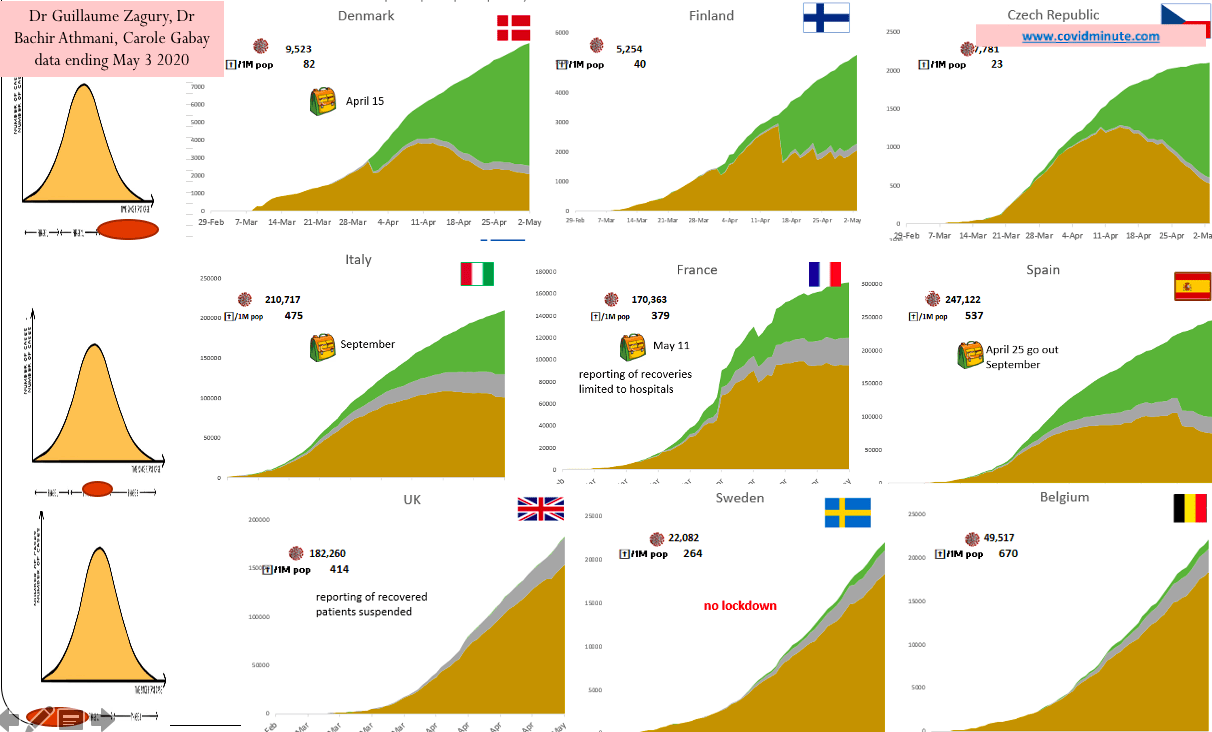
I.4 Europe: A Europe has 3 speeds: peak passes (deconfinement) – plateau – epidemic phase
I.5 World: Russia, 2nd country in terms of incidence and Brazil 3rd:

I.6 World: Earnings Indicator
– comparative international results of “country strategies”
– Indicator certainly not perfect (because of the tests, population density, the median age of the country) but available, to assess the impact of “Country” strategies.
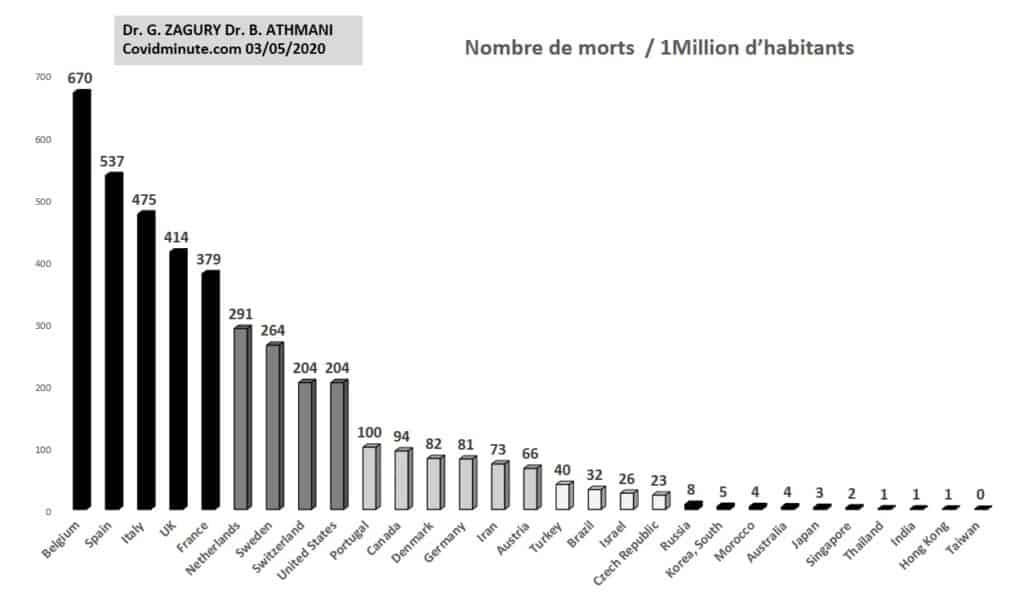
Beware, however, of too hasty comparisons (cf Finland has low population density versus Singapore)

II. 360-degree analysis
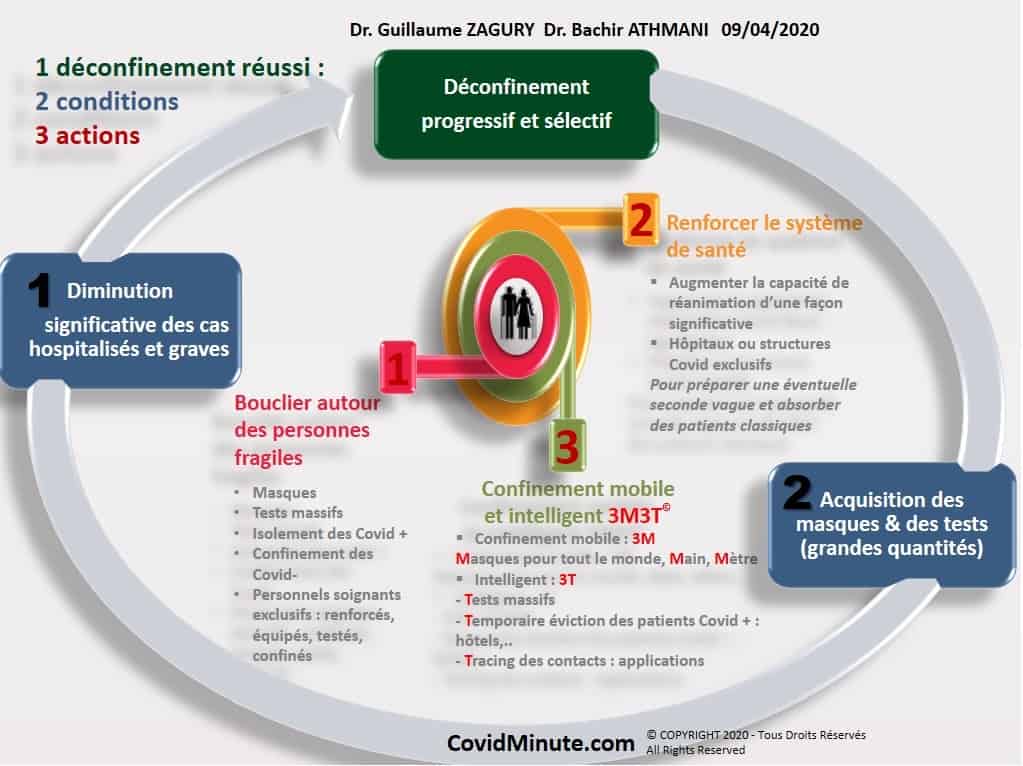
Ⅱ. A The Government follows to the letter (2 conditions,3 actions) our deconfine scheme (since 9 April)
… But recommendations have not yet been implemented.
Ⅱ. A.1 The 2 medical conditions: epidemiological and resuscitation beds available
Epidemiological: Active circulation of the virus
Currently, the indicators are relatively similar to the historical map of pre-containment (Great East and Oise). And so it can be falsely reassuring for the future, as we have experienced.
.

Resuscitation capabilities: this is a major point.
I thank my former colleague Jerome, with whom I shared a conversation yesterday, in order to offer you a shared and objective vision:
Already almost tense flow in pre Covid (see savings plan and a resuscitation bed is expensive – plus 4000 euros/day). Some services on the outskirts of Paris are likely to be permanently red (more than 80% occupancy rate and even more some WE).
The hospital had “pushed the blackberries” as my colleagues say, in order to absorb the C wave: capacity in USI/Resuscitation beds increased from 5,000 to 9,000 beds (see Covid diagram in one minute)
The system had been able to contain the wave in extremis, thanks to System D (see transfer to the West and abroad).
Currently, regular patients (coronary heart disease, insufficient respiratory, attempted suicide, etc.), are beginning to return to the wards with qualitatively more advanced forms due to the low surveillance for more than a month.
The Hospital therefore closes Covid beds to include C (-) in need of surgical care (e.g., re-opening of the recovery rooms previously used for intensive care Cs).
Similarly, clinics resume their normal activities and no longer accept C patients in hospital or resuscitation.
As a result, at the time of deconfinment, our ability to hospitalize Cs in ICU/resuscitation decreases, and will not be immediately reversible (C patients occupying beds).
Ⅱ. A.2 Hence our proposal of a pro-active attitude, from a month ago (!)
In Ile-de-France, so as to anticipate the 2 waves C (-) and C () and not suffer:
Unlike the Germans who have a 10k bed “mat” ready to absorb a massive influx, France is not at this level of preparedness.
We persist, for the creation of a structure of 500-1000 C beds with USI and resuscitation beds in the epicenter “Ile de France” (Val de Grace, Hôtel Dieu, periphery…), to free the other hospitals and treat the Cs. Transfers to France or abroad would be extremely time-consuming.
Do we have the human capacity (the stake) and material (our manufacturers will soon put 10 k respirators on the market and it will be necessary to ensure the pharmacological supply type curarizing …) to realize it is a question to ask.
This is based on our observation of what happened in Wuhan, where everything was unblocked with the construction in 3 weeks (around 2 February) of two structures of 1000 beds (with 5G!), for isolation and treatment of patients C () in parallel with the reinforcement of 30k health professionals.
If we are to use it to relieve an epidemic overheating system (see 2nd potential wave), we will have been ahead of the virus, and if we do not use it, it will be even better, meaning that the barrier measures (“3M”: Mask-Main-Meter) and the measures of management (3T: Test-Tracing-Transfer/isolated) have been effective (but
I think that this proposal from the Covidminute team (launched at the end of March!) is making its way, and that it will be taken up by journalists, health professionals, and other decision-makers in the near future.
To follow…
Ⅱ. A.3 Protecting the Vulnerable and Professionals: The Key to a Successful Deconfine
Ephad (9312 deaths to date, or 40% of mortality) are potential viral incubators (see episodes of the Diamond Princess, see CDG), and special attention must be paid to them (remember that the average age of death is over 80 years).
We are all waiting for a war plan for the Ephad (or equivalents) who are touching. Let us be sure that the government will act in this direction by providing the clear elements of protection: FFP2 masks and personal protections, testing of caregivers and members, policy of isolation in case of C, …
The same is true of patients with associated high comorbidity who need preventive logistical support (FFP2 mask…)
Ⅱ. A.4 Regarding tracing and isolation: probably over-liberticidal judges
As he will be a liberticidal judge, we will not be able to access contact cases not electronically (XXIth century), but more in the traditional way through interrogation.
As a result, put liberal physicians back on the front line, giving them the tools to diagnose, try to trace C cases and follow them.
Similarly, the conditions of isolation, drastic in Confucian Asia (cf high population density: 130 people per km2 in France versus 7900/km2 in Singapore), will probably be much more flexible in France (in our eyes, isolation in an ad-hoc structure is nevertheless an imperative.
Ⅱ. A.5 When the 2 epidemiological conditions and preventive action on populations at risk are met, it is not necessary to go into the excess of the “ayatollahs” of hygiene
For the reasons known: economic, medical (C-) and mental health, it is necessary to deconfinate.
“Living with”: with the “3M” tools of the individual protective barrier, and with a gradual resumption of school and professional activities. For example, in China, there is no time limit for meeting healthy people.
In the meantime… that an effective vaccine makes its way (natural immunity is apparently slower and discussed)
Ⅱ. B. France, regional vision
Ⅱ. B.1 Hospitalizations: Space Time Evolution
Ⅱ. B.2 Resuscitation beds: réanimation containment is effective
Ⅱ. B.3 Map of deconfinement (synthesis of the two indicators): an East-West and North-South gradient

Ⅱ. C WORLD: Russia in epidemic phase and Africa surprises us
With the contribution of Dr. Bachir Athmani, Stéphane and Alison, companions of the first hour, whom I thank again for their unwavering support.
Beware of certain figures (number of cases, deaths…) that are highly questionable because they vary from country to country (e.g. availability of tests), with measurement biases and therefore major under-reporting in some countries.
Ⅱ. That’s what I’m going 1 Prevalence: 2,159,000 active cases confirmed for observation

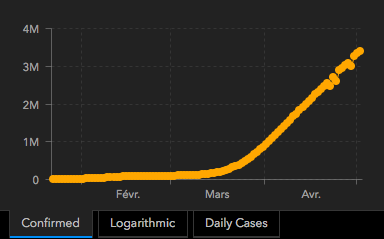
Epidemic growth since January 1: More than 3 million cumulative cases
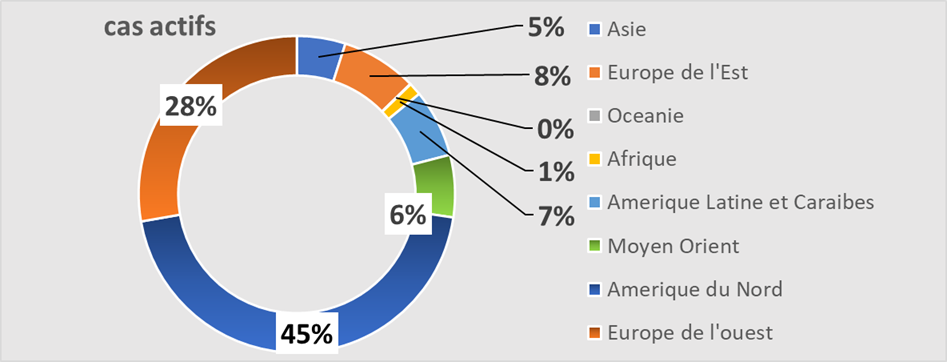
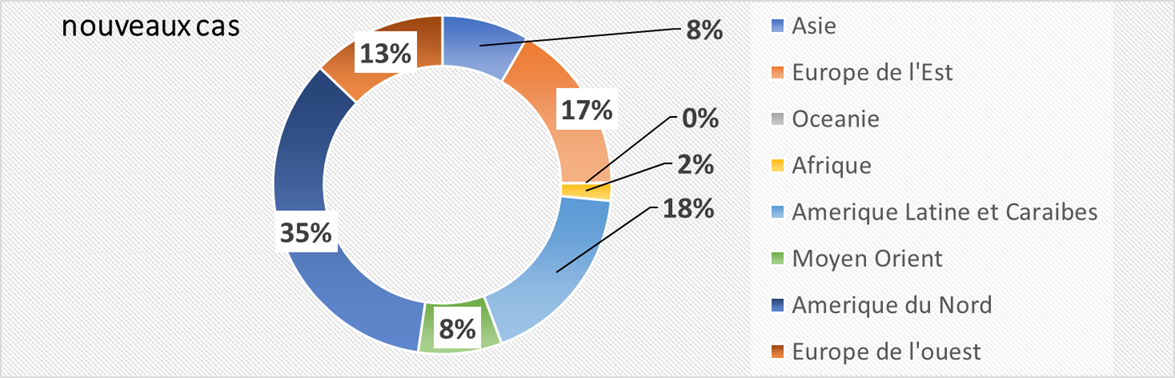
Geographical vison: 4 active poles: Americas, Europe, Middle East, Russia.
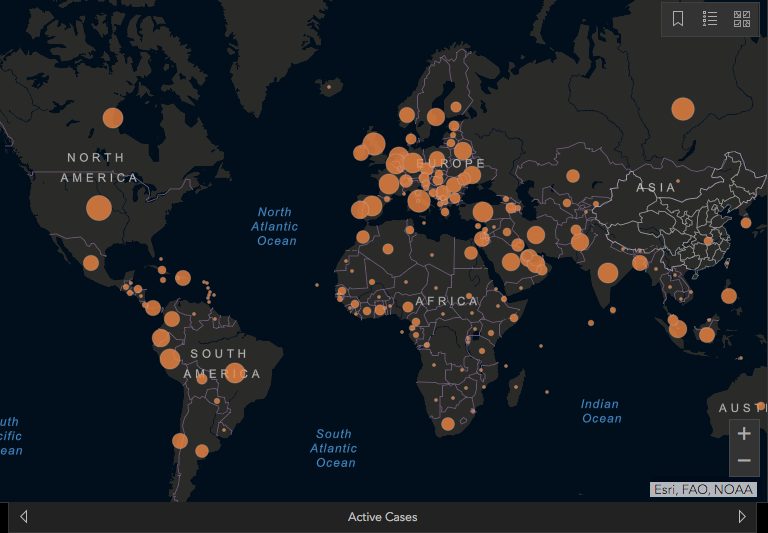
Note the very low number of deaths (example 15 deaths reported so far in Cote d’Ivoire) or cases of resuscitation in Africa (if resuscitation were full we would be): effect temperature/humidity, youth of populations, effect “quinine” … many questions still to be decided.
By continent: Americas, 50% of reported active cases, Europe 30%, Middle East and Russia has 7%
Top 10 countries
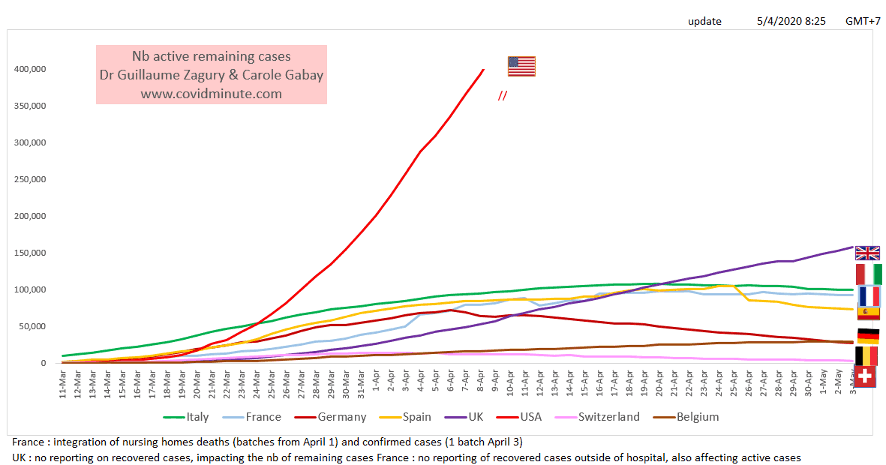
United States 939k (yesterday 931k)
United Kingdom 158k (yesterday 154k)
Russia 117k (yesterday 108k)
Italy 100k (yesterday 101k)
France 93k (yesterday 93k)
Spain 73k (yesterday 74k)
Turkey 60k (yesterday 63k)
Brazil 51k (yesterday 49k)
Netherlands 35k (yesterday 35k)
Peru 31k (yesterday 29k)
Ⅱ. C.2. Incidence: 78,000 new cases detected yesterday and Russia has an increasing rate of new cases.

Depending on the weather:
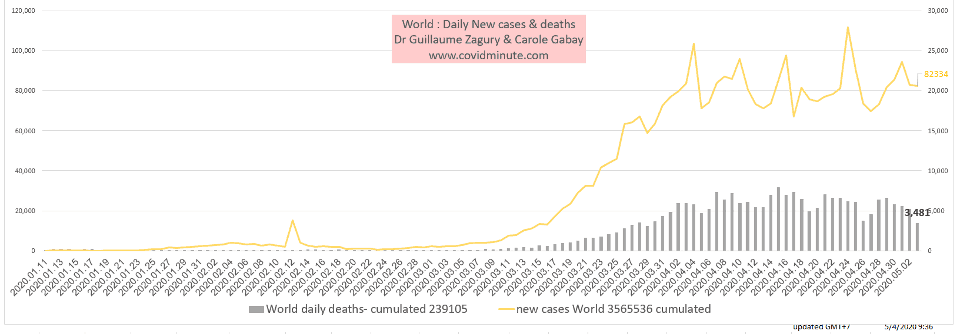
Ⅱ. C.3 Incidence: 78,000 new cases detected yesterday and Russia has an increasing rate of new cases.
Geographic:
- By country
USA 25k (28k yesterday)
Russia 11k (10k yesterday)
Brazil 5k (4k yesterday)
United Kingdom 4k (5k yesterday)
Peru 3k (2k yesterday)
India 3k (2k yesterday)
Canada 3k (2k yesterday)
Spain 2k (3k yesterday)
Turkey 2k (2k yesterday)
Pakistan, Singapore, Iran, Saudi Arabia, Qatar, United Arab Emirates, Bangladesh, Belarus, Ukraine, Germany, Italy, Mexico, Chile, Ecuador: 1 to 2k
Ⅱ. C.4 Historical Vision of the Epidemic
In 4 months, the nanoparticle has spread all over the planet and has affected all sectors of activity (health, economic, social, political …)
Health: 4 billion confined, nearly 3 million historical cases reported, 2 million active cases reported (and 240 k deaths)

The West is the first victim of the virus.
Keep in mind the “3M reflex” (Hands-Masques-Metre) to protect yourself… but above all to protect the most vulnerable.
Confidence and solidarity for this collective struggle
Dr Guillaume ZAGURY
- “Allsuccess is collective,”thanks to:
- The entire “Medical” team of “GCMN” type (Global Covid Medical Network): Dr. Bachir Athmani, Dr. Marc Abecassis, Dr. Mohamed Fadel, Dr. Ibrahim Souare, Dr Jonathan Taieb…) that make this project a muste,
- The entire data analysis and IT team: Carole Gabay (“Data Analysis Expert”), Richard Coffre (exceptional webmaster), Flavien Palero (digital manager), Mathieu Bouquet (for his past contribution)
- The whole “Communication” team (Flavien Palero, Laetitia, Marie, Alison…): without whom this project would not have been possible.
- All the historical financial patrons (Jérôme, Benjamin Denis and the B Square Consulting Company, Benoit Rossignol, Arnaud Bricout and TAG Advisory and Gilles Langourieux…) who work for “Citizen Actions”
- We also thank the Paul Foundation
- If you feel like a patron or partner to finance computer development (all the others have been volunteering for 88 days!), please contact me (guillaume 888@hotmail.com).
- Also, our team, although partly based in Shanghai, will be delighted to welcome you … because it’s not the work that’s missing…!
[DISPLAY_ULTIMATE_SOCIAL_ICONS]
