
We know that many journalists and decision-makers (“crisis cells”, ministries, …) read this analysis “served at breakfast”, and we are delighted. We just ask you, when you use our ideas or illustrations, to have the courtesy to quote us.
Doctor Guillaume Zagury, based in Shanghai, specialist in international public health and in health innovations, comments for the Community day by day the evolution of the epidemic for more than three months, and delivers in preview the elements of understanding on its “country & region analysis” and foreseeable consequences (experiences of SARS in 2003 and of Covid-19 in China).
A whole remarkable multidisciplinary volunteer team allows the realization of this analysis which wants to be factual and objective (moreover, do not hesitate to join us: mail below): “all success is collective”.
Beyond the volunteer skills, this project was made possible by the support of our patrons with a civic vision: the Paul Bennetot Foundation (Matmut Foundation under the aegis of the Fondation de l’Avenir), B Square, Tag Advisory , Daxue Consulting, as well as various fellow travelers (Jérôme, Dr Benoît Rossignol, Gilles Langourieux, …)
All of our illustrations created almost 100 days ago will soon be available on our site and you can download a large part of them. (www.covidminute.com).
I. COVID “360 ° MINUTE”: graphs and maps (=> 80% of the information)
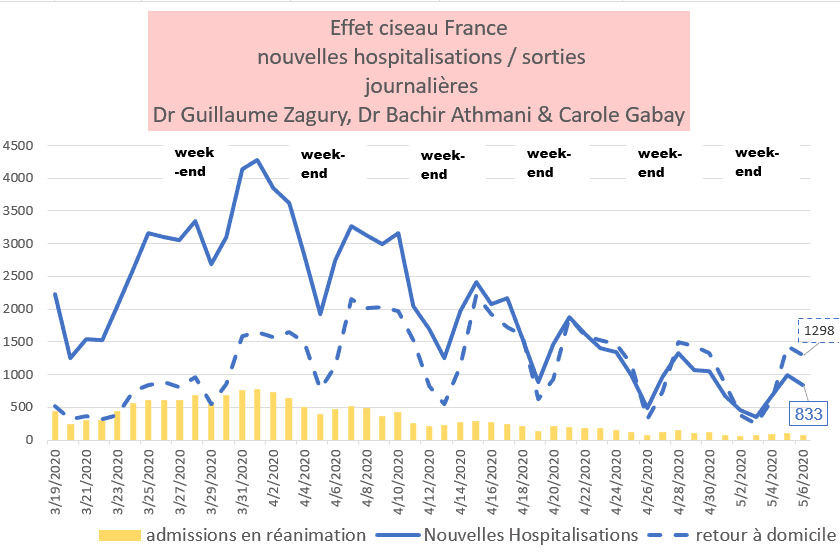
I.1 France – after 47 days of confinement, a favorable but slow dynamic
Scissor effect in progress (hospitalizations and resuscitation): note that if the dynamics are there, the number of daily hospitalizations despite confinement is still high (more than 800 / day)
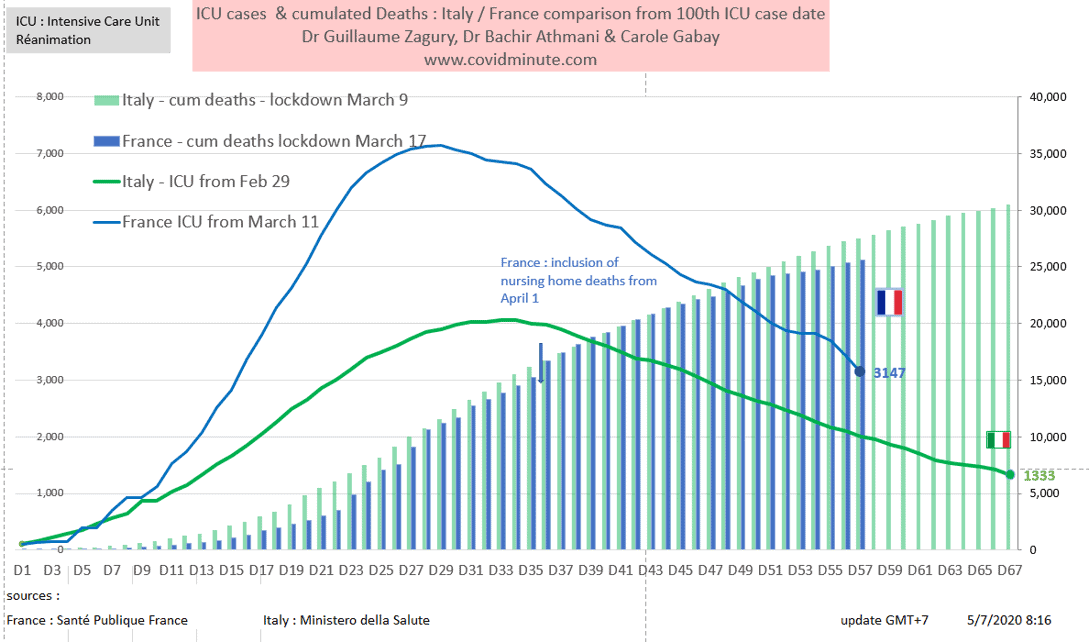
I.2 Time vision: we are following Italy 10 days later
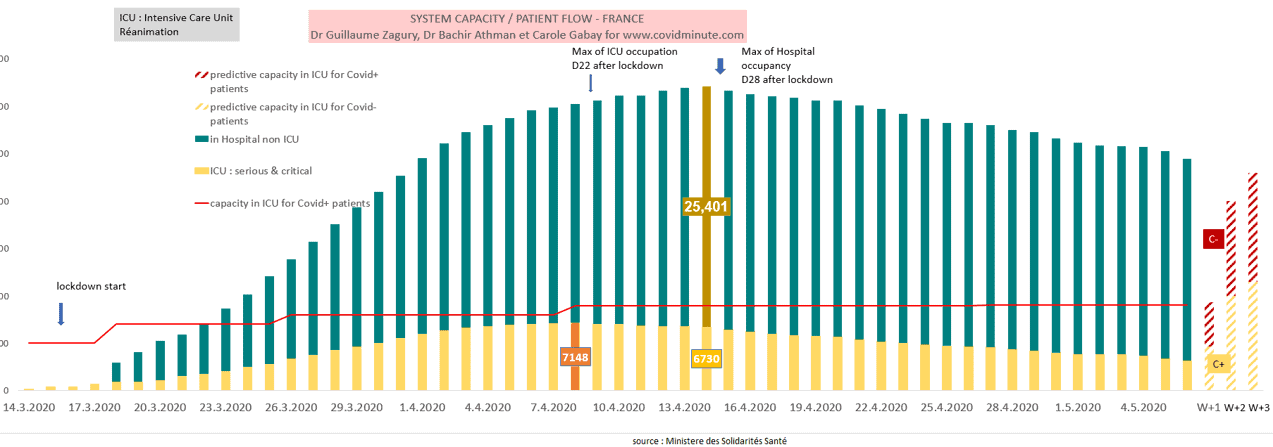
I.3 France – Provisional: resuscitation beds available (the stake from May 16
Covid beds (+) below 4000 today (3147 versus 3430 yesterday) with a maximum capacity to date estimated at 9000 beds.
Post-deconfinement projection, based on 3 elements: historical data, incubation time (D7 with an expected increase around May 16), and the influx of patients C (-) (around 3200 out of 7183 beds occupied)
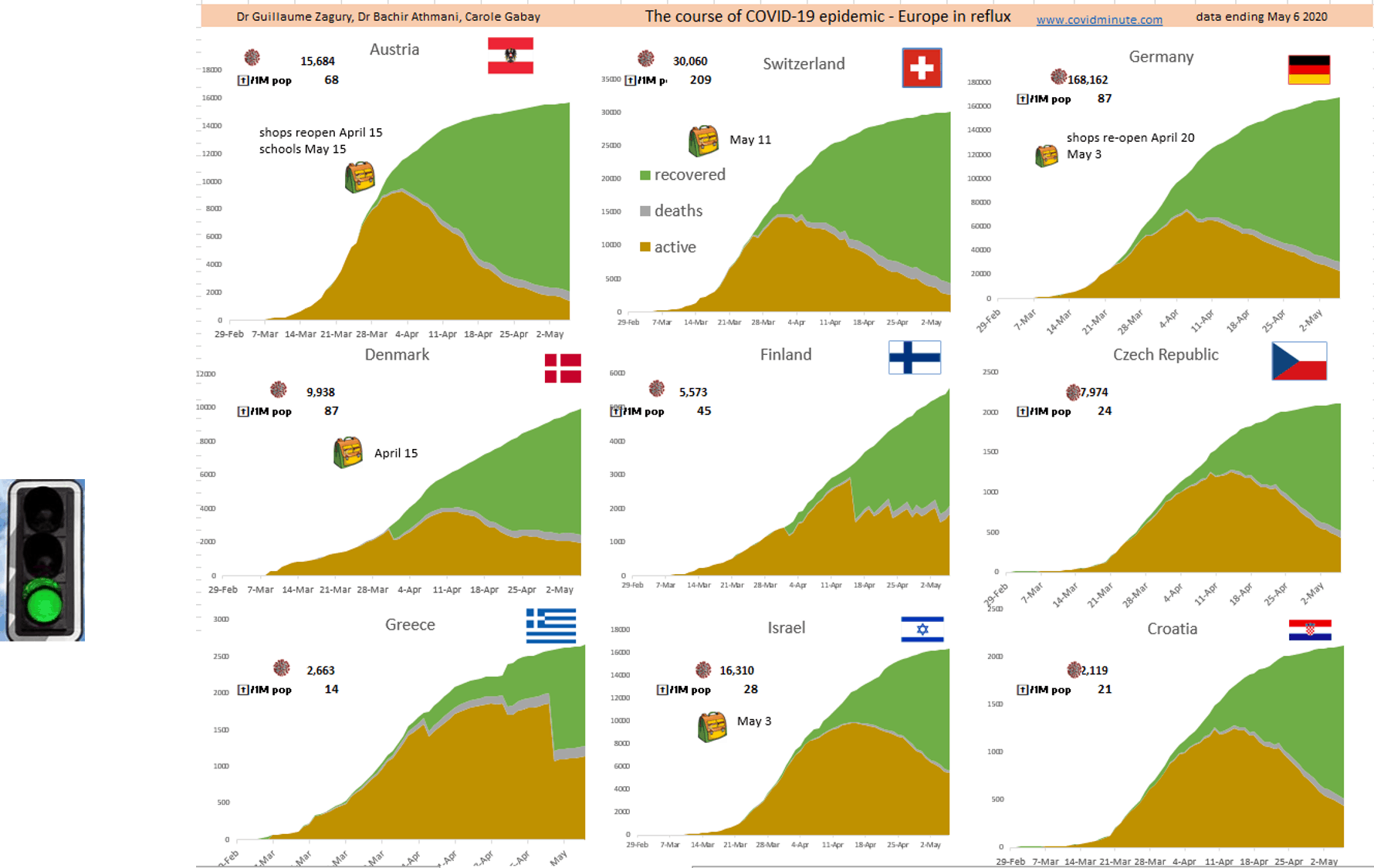
I.4 Europe: a 3-speed Europe: past peak (deconfinement) – plateau – epidemic phase.
Note that in France, the cured Ehpad patients or patients not hospitalized, are not counted in the “cured”, and consequently, the decline (importance of the “green”) of the curve is actually stronger than the vision “ graph ”.

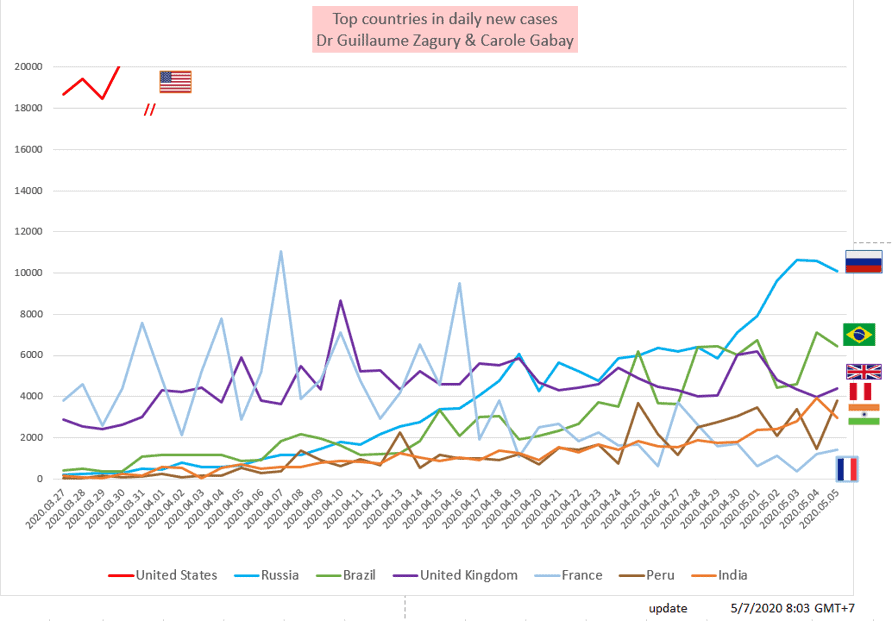
I.5 Mapping of the epidemic (active cases declared): 4 active foci: USA / Latin America / United Kingdom / Russia
I.6 World: More than 10,000 new cases yesterday in Russia and Brazil
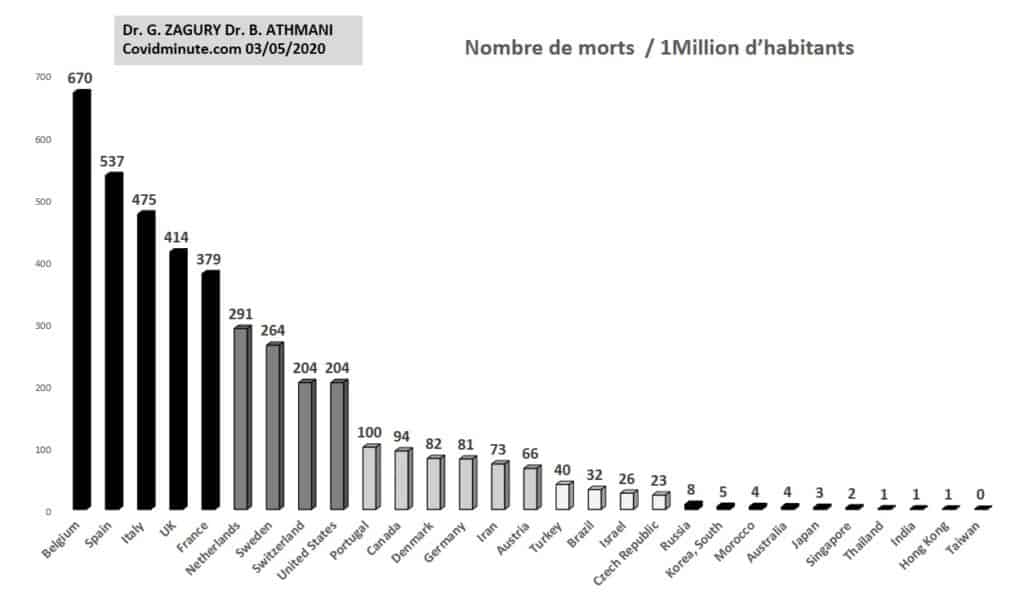
I.7 World – result indicator – mortality / 100k individuals: 3 levels observed
Comparative international results of “country strategies”
Indicator certainly not perfect (because of the tests, population density, median age of the country, etc.) but available, to assess the impact of “country” strategies.
However, be careful with overly hasty comparisons (see Finland or Australia with a low population density versus Singapore or New York)
Figure updated weekly
II. 360 ° analysis
With the collaboration of Dr Bachir Athmani
II.A Serene look to the future
II.A.1 Healing: more than 98% of infected people recover favorably
In the vast majority of cases it is an infectious pathology which heals favorably with at least 98% of clinically infected patients
80% of people infected will be mildly or not symptomatically (unlike the seasonal flu which generally keeps you at home for 5-7 days).
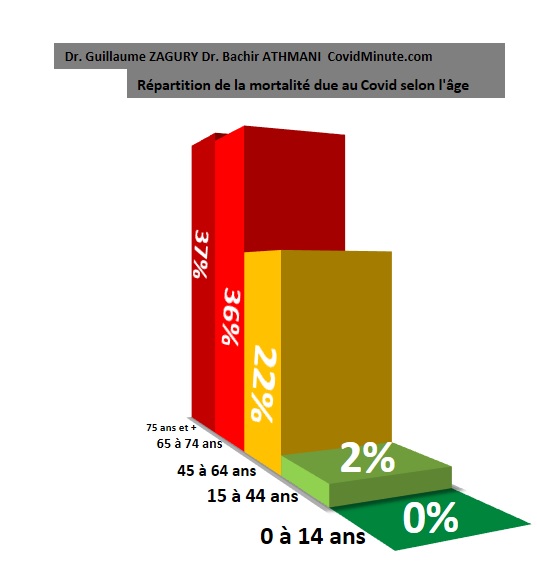
In subjects without a major risk factor (age, comorbidity), i.e. around 80% of the population, less than 1% of mortality in the event of infection (rate observed in Shanghai when the health system is not under stress).
In practice, we are not in an Ebola-type atmosphere (50% mortality) and if people at risk (20% of the population) are well protected, we must remain calm and confident: the episode of Charles de Gaulle confirms that 100% of young, healthy adults emerge unscathed from the infection (less than 1% in intensive care and 0 deaths out of more than 600 cases).
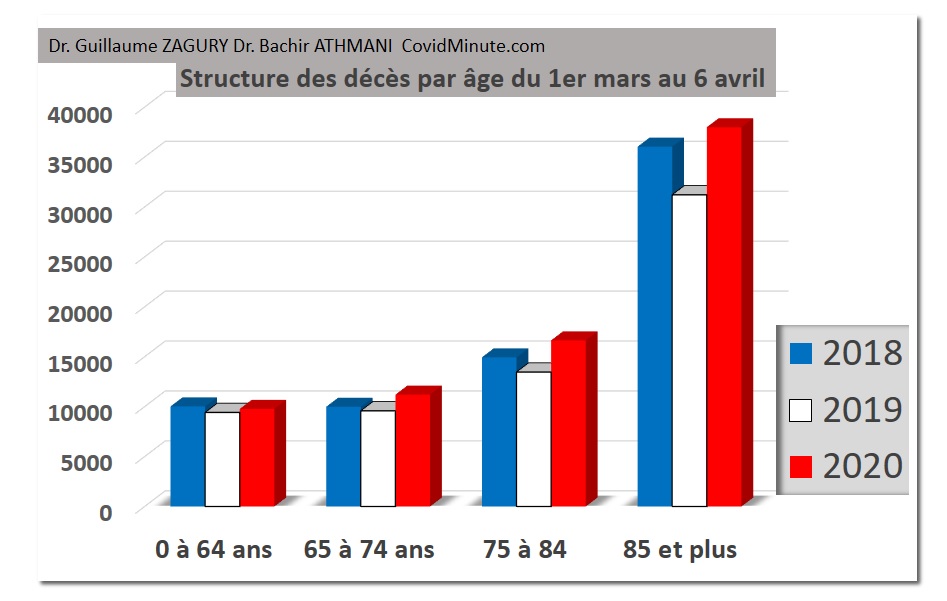
As this graph shows over the past 3 months, there will probably be no impact on macroscopic indicators of the overall mortality type; gain of years of life lost among young people by a reduction in road accidents or work accidents, but excess mortality of the elderly, in particular men (life expectancy normally around 80 years), following the Covid catalyst or the delay Covid Patient Management System.
II.A.2 Spared children
If the disease is contagious (family cases ++), children are most often asymptomatic (“healthy carriers”) and absence of death in France among children under 15 years of age.
II.A.3 Existing effective solutions: collective and individual (“3M”)
At the collective level: if the confinement had not taken place on March 19, our health system (resuscitation beds available) would not have been able to cope and the results would have been much heavier.
In the absence of pharmacological solutions, individual barrier measures have proven their worth:
3M (Hand Mask -Meter- since February 2, 2020), for the vast majority of us in the event of social life
4M (add “Minute”: limitation of physical contact times): for people at risk (18 million), or carers.
II.A.4 Caregivers at their top level
It was the soldiers on the front who saved the general staff from the initial shortcomings.
The system has managed to hold up and must remain vigilant for the future (and particularly after May 18).
II.A.5 Exponential fundamental knowledge which should lead to concrete therapeutic results
“Wars” have always generated disruptive innovations by mobilizing collective intelligence. Currently, the teams are evolving at a global level, with 24/7 projects.
Recently, a French team proposed a therapeutic solution based on monoclonal antibodies (interleukin 6), which is still being evaluated.
Regarding chloroquine (the scientific debate is not yet settled), note the very low mortality rate observed in pharmacovigilance in certain countries such as Switzerland or Morocco.
For the vaccine, many structures are in competition including 4 Chinese and of course the team of Professor Gallo in Baltimore.
II.A.6 Possible hopes in the short and medium term due to the physical environment inherent in the virus:
RNA viruses are generally of better prognosis than DNA viruses.
The host animal of the virus is wild (bat in principle), as for SARS (see animal civet), and is not domestic (see dromedary for MERS, see avian or swine viruses for influenza). This would therefore be less favorable for easy recrudescence, with the risk of a strong mutation of the virus.
The notion of temperature (/ humidity) could impact for this respiratory virus:
at the historical level: the case of SARS suddenly disappeared in spring 2003
at the geographic level: 90% of the cases observed belong to a geographic belt, and the same observations of North / South gradients in certain countries such as Vietnam.
Similarly, it would be a possible hypothesis (with the young age of the populations) to explain the absence of an epidemic outbreak in certain countries such as: Africa, India, Indonesia, Australia, Thailand, … but conversely 10,000 new cases identified yesterday in Brazil (even if in the winter season).
II.B Europe: countries that have deconfined
II.C France – evaluation
II.C.1 Persistent scissor effect
With nevertheless still nearly 1,000 hospitalizations per day despite 46 days of confinement:
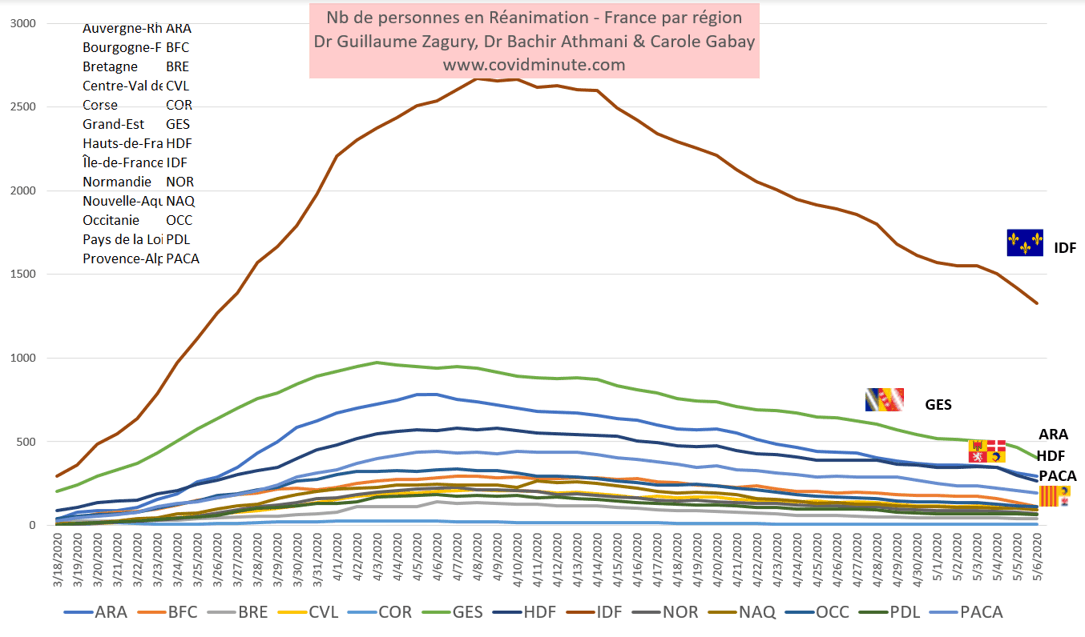
II.C.2 Resuscitation empties of their C (+) patients in the different regions:
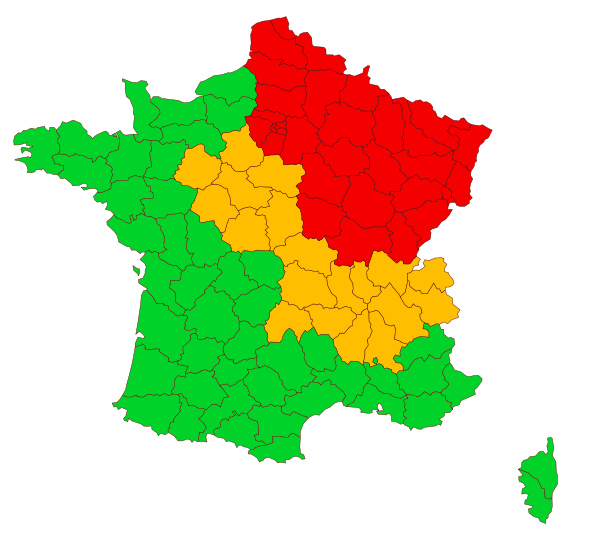
II.C.3 Preparation for deconfinement – departmental vision:
27 departments always in red and East-West and North-South gradient
Departmental vision of combinations of the 2 factors: density of cases and available resuscitation beds (red: 2 negative indicators – orange 1 indicator – green: 2 positive indicators)
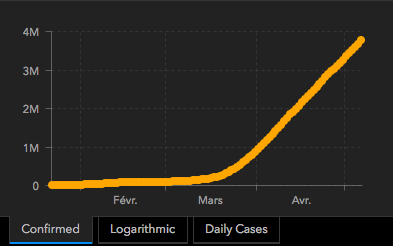
II.D WORLD: the threshold of 4 million declared cases crossed (240k official victims)
With the contribution of Dr Bachir Athmani, Stéphane and Flavien Palero, companions from the start, whom I thank again for their unfailing support.
Beware of certain figures (number of cases, deaths …) which are extremely questionable as they vary from one country to another (example: availability of tests), with measurement bias and therefore a major under-declaration in certain countries.
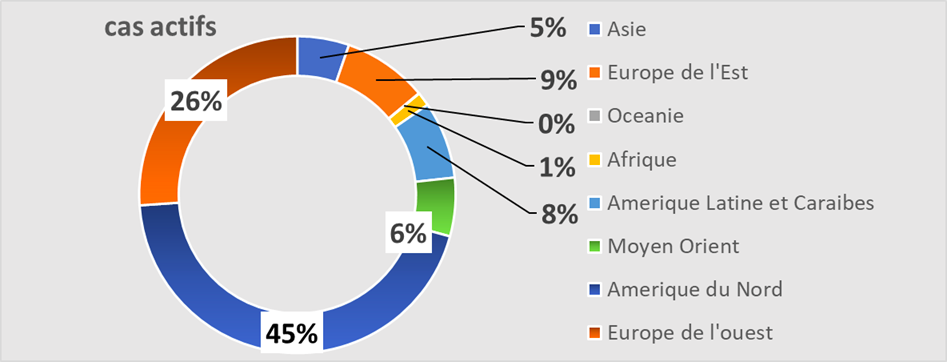
II.D.1 Prevalence: 2,259,000 active cases confirmed under observation
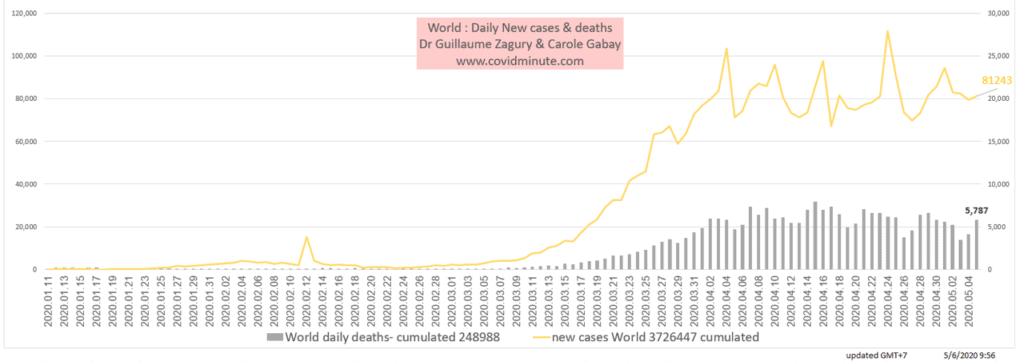
Epidemic growth since January 1: around 4 million cumulative historical cases
Source: John Hopkins University
Geographic vision: the world (4 million cases declared historically) is equivalent to a multitude of Wuhan (approximately 40k cases declared)
Source: John Hopkins University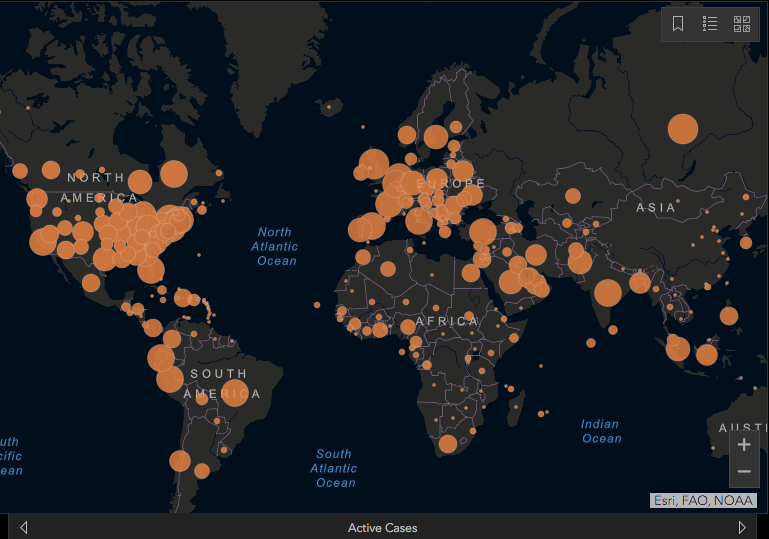
By continent: West 80% – Russia and Middle East: 10% – Africa 1% of reported cases
Top 10 countries: see full country table on: covidminute.com
United States 977k (yesterday 965k)
United Kingdom 171k (yesterday 165k):
Russia 143k (yesterday 134k)
Italy 92k (yesterday 98k)
France 94k (yesterday 92k): note that France is reinstated in the “Top 5” following administrative updates
Spain 68k (yesterday 70k)
Brazil 68k (yesterday 59k)
Turkey 50k (yesterday 53k)
Netherlands 36k (yesterday 36k)
India 36k (yesterday 34k)
Peru 36k (yesterday 34k)
II.D.2. Impact: BRIs (especially Brazil-Russia) in epidemic phase
Incidence: 86,000 new cases detected yesterday
Depending on the weather :
Geographic:
By continent: soon more new cases in Russia than in Europe
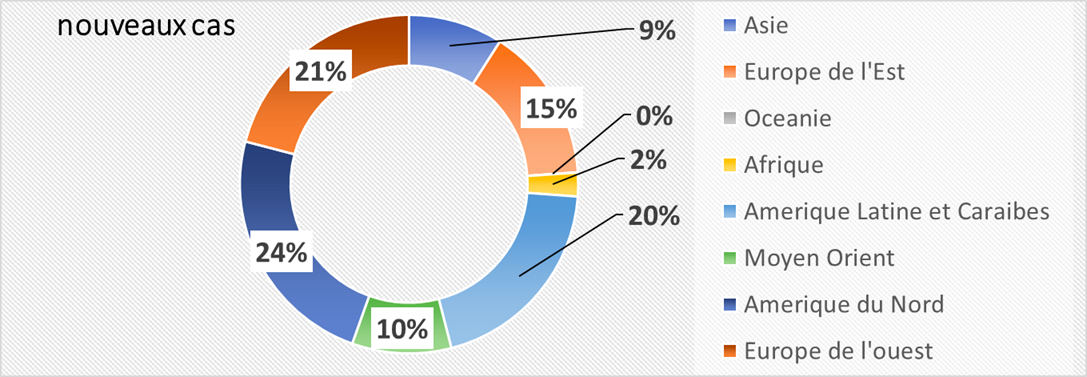
By country: more than 10k new cases reported in Brazil and Russia
United States 19k (23k yesterday)
Russia 11k (10k yesterday)
Brazil 11k (6k yesterday)
United Kingdom 6k (4k yesterday)
France 4k (1k yesterday)
Peru 4k (4k yesterday)
India 4k (3k yesterday)
Spain 3k (2k yesterday)
Pakistan, Singapore, Iran, Saudi Arabia, Qatar, United Arab Emirates, Bangladesh, Belarus, Ukraine, Turkey, Italy, Sweden, Ghana, Canada, Mexico, Chile: 1 to 2k
II.D.3 Time-space vision: for the followers of detailed analysis:
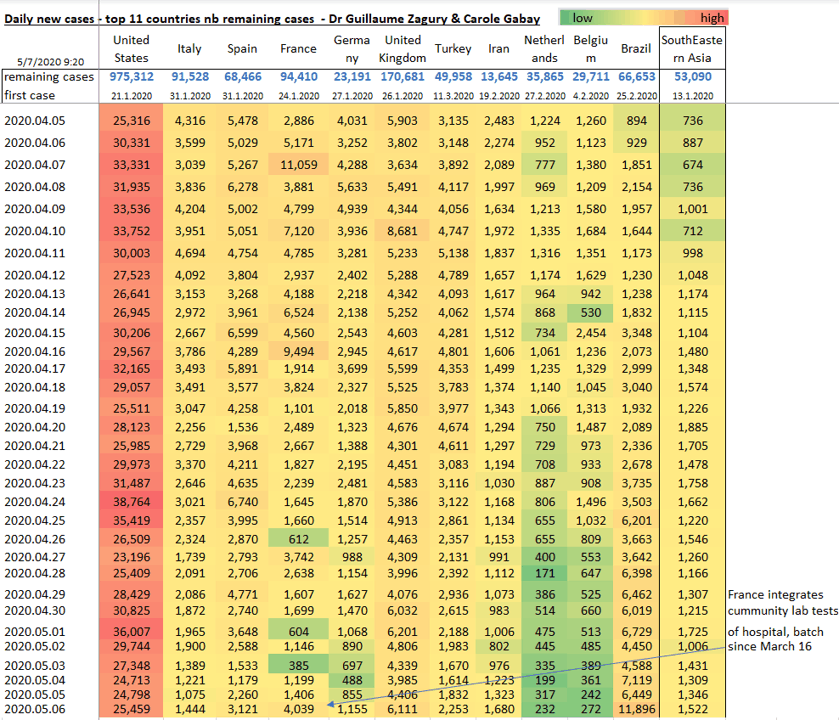
All the tables of our Data Analysis Expert, Carole Gabay, on the site: www.covidminute.com, in the “Resources” section.
III. TOMORROW
Mortality study: raw and relative figures via different World Maps,
Keep in mind the “3M reflex” (Hands-Masks-Meter) to protect yourself and the “4M reflex” (Hands-Masks-Meter -… Minute) for fragile people (& nursing staff)
… But above all to protect the most vulnerable.

Trust and solidarity for this collective fight
Dr Guillaume ZAGURY
“All success is collective”, thanks to:
the whole “Medical” team of the “GCMN” type (Global Covid Medical Network): Dr Bachir Athmani, Dr Marc Abecassis, Dr Mohamed Fadel, Dr Jean Michel Serfaty, Dr Ibrahim Souare, Dr Jonathan Taieb, ,, …) that allow this project to exist,
the entire data analysis and IT team: Carole Gabay (“Data Analysis Expert”), Richard Coffre (exceptional webmaster), Flavien Palero (digital manager), Mathieu Bouquet (for his past contribution)
the entire “Communication” team (Flavien, Laetitia, Marie, Alison …): without whom this project would not have been possible.
all historical financial sponsors (Jerome, Benjamin Denis & Société de Consulting B Square, Benoit Rossignol, Arnaud Bricout & TAG Advisory and Gilles Langourieux, Sabrina Rocca, …) who work for “Citizen Actions”
We also thank the Paul Benetot Foundation
If you feel like a patron or a partner to finance IT development (all the others have been volunteers for 88 days!), Don’t hesitate to contact me (guillaumez888@hotmail.com).
Also, our team even if partly based in Shanghai, will be delighted to welcome you … because there is no shortage of work …!
[DISPLAY_ULTIMATE_SOCIAL_ICONS]
